I continue to annoyed by all the fear-mongering in the industry around what CVS Caremark is “doing to their employees”. What about focusing on how they are helping their employees to get better? (If interested, you should read some of the information they have on their blog.)
Our “Plan for Health” combines an evolving, best-practice approach to health coverage with preventive care and wellness programs. Our colleagues will be more accountable for taking control of their health and associated costs. The first step is getting to know your numbers by getting a health screening and completing an online wellness review each year. If colleagues complete both by the May 1, 2013 deadline, they will avoid paying an additional $600 for the 2013-2014 plan year. (from the CVS Caremark blog)
I was hopeful to hear someone come out strongly and speak about it yesterday on CBS, but instead the CEO of Mercer just talked about “soft” programs that depend upon consumers being proactive around their health. I would rather hear about the value of screenings and how it helps employees. In talking with one friend of mine at a biometrics company, he told me that in one case almost 40% of the people that they identified with diabetes (or pre-diabetes) and hypertension (or pre-hypertension) didn’t know they had the disease (or were at high risk). That to me is a valuable insight to the individual especially when coupled with a program to help them learn and manage their disease (or risk).
For example, companies for years have been using Health Risk Assessments (HRAs) to try to baseline employee health and use that to accomplish several things:
- Help the employee to understand their risks
- Identify people who should be in coaching programs to improve their health
- Learn about their population and how to improve their health benefits
Use of biometrics is the right evolution from the HRA. People have tried HRAs for years with some success. Companies pay as much as $600 for people to take this online survey that has no necessary link to reality. Most HRAs aren’t linked to lab values. Most HRAs aren’t linked to claims data. Most HRAs don’t necessarily trigger enrollment in health programs. They are supposed to activate the employee to be proactive which doesn’t work for many sick consumers especially those in the “pre-disease” phase. (Here’s a good study that does show some increased activation.)
As I mentioned the other day, this use of biometrics and link between incentives and participation (and ultimately outcomes) is normal and will ultimately improve the link between the workplace and the employee around health.
Let’s take a broader look at insurance to help set some context:
- For life insurance, you have to disclose certain data and depending on the policy level you have to do other things like get a physical and have blood work drawn. That effects your costs and their underwriting.
- For car insurance, if you get in accidents, your costs go up. In some case, you can have a monitoring device put on your car to lower your costs. (like getting blood work done)
- For home owners insurance, your costs go up if you live in a flood zone or a earthquake zone. It also goes up if you have lots of claims.
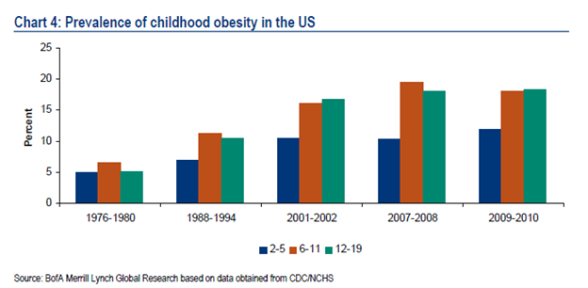
Whether we want to admit it or not, we do determine a lot of our healthcare costs based on decisions we’ve made or had made for us since we were kids. Some of these are conscious and some are subconscious. And, obesity which is a large driver of many of these chronic conditions and has an impact on your likelihood of having cancer. So, a company asking for your BMI and other data to help understand your risks for healthcare costs (of which they typically pick up 80%) doesn’t seem unusual.
Certainly, some are environmental such as those that live in “food deserts” like Detroit. In other cases, workplace stress can affect our health. We’re just starting to get smarter about “sitting disease” and it’s impact on our health. Or, we may take medications that affect our blood pressure (for example). It’s certainly important to understand these in context of your lab values and discuss a holistic strategy for improving your health with your physician and any care management resources which are provided to you (nurse, social worker, nutritionist, pharmacist).
This idea of learning more about employees in terms of biometrics, food, sleep, stress, social interaction, and many other data points is going to be more and more of a focus. Companies want to learn how their employees do things. They want to understand their health. They want to improve their health. They want to invest in their workforce to improve productivity, innovation, and ultimately job satisfaction.
While the glass half-empty people won’t see this and there are some companies that don’t always act this way, I generally believe that companies are trying to act in a way to increase their top line and most intelligent executives understand the correlation between health and wealth and the link between employee satisfaction and growth.
Ultimately, healthcare costs are estimated to put a $240,000 burden on us after we retire (even with Medicare) so if someone wants to help me become healthier and thereby save me money which improves my ability to retire and enjoy life I’m happy for them to do.

 September 18, 2013
September 18, 2013