January 30, 2013
January 30, 2013 
While prescription adherence continues to be a $290B+ problem, we still address the problem in a drug by drug approach due to silos within our healthcare value chain.
For example:
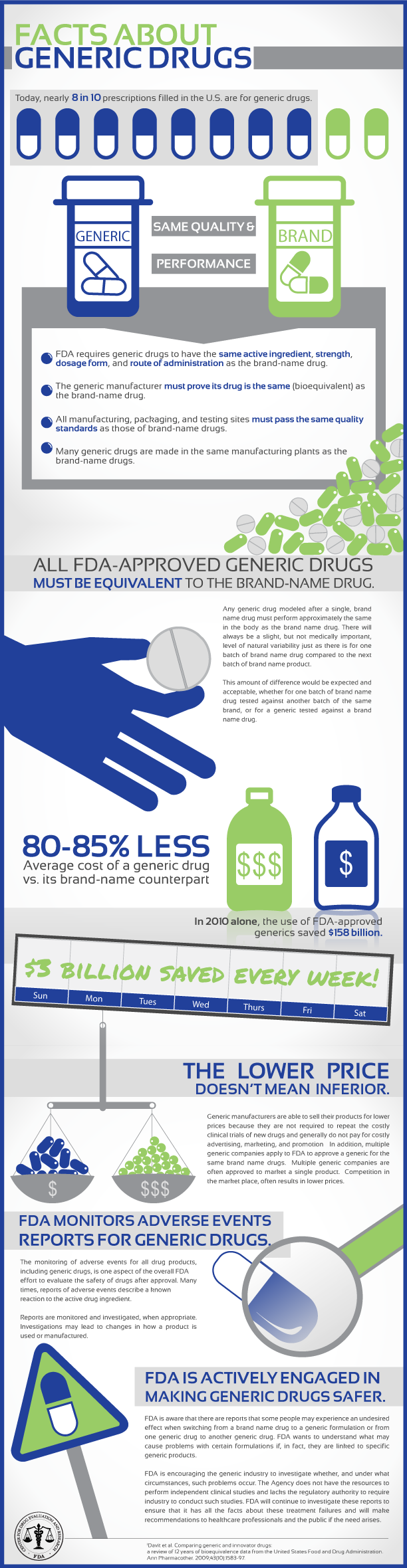
- Generic drugs (about 80% of the prescriptions filled) are the lowest cost and most profitable drugs (to the suppliers). For these medications, you’ll usually have several programs:
- Refill reminder calls, text messages, letters
- From the PBM
- From the retail pharmacy
- From the mail pharmacy
- Refill reminder calls, text messages, letters
- Auto-refill programs
- Brand drugs are usually higher cost and profitable (to the manufacturers). For these, you have pharma funded programs such as:
- Messaging attached to your bill at the pharmacy
- Letters sent to your house by the pharmacy
- Specialty drugs which are the highest cost and typically profitable (across the supply chain). For these, companies often take a higher touch approach:
- Pharmacy techs calling you
- Nurses calling you
Additionally, there is additional effort made to keep you adherent if:
- You’re a Medicare Advantage member in one of the categories where adherence is measured for the STAR metrics program
- You’re have a condition where adherence is a key metric for HEDIS or some other quality program
For those of us that have studied adherence, you know that this is a multi-factorial issue meaning that there are numerous things that impact your adherence. Some people will respond to nudging. Some people need to better understand their disease. Some people need co-pay relief or patient assistance programs. Some people need a different medication.
But, the two things we don’t need are:
- Being treated like a disease not a patient
- Getting 4, 5, 10 different communications from different parties on different schedules
So, what’s the answer. There isn’t a silver bullet (which is what we’d all like). I believe the best alternative is to drive adherence through the disease management and case management companies. These nurses are treating the patient. They are discussing their multiple co-morbidities with them. They are talking about and understanding their barriers. They should be able to help “prescribe” information and tools to help them with their adherence.
Of course, the issue here is engagement. If we’re only getting 10% of the patients with chronic illnesses to participate in our programs (which is about the national average – I believe), what about the other 90%. This is where a care coordination program that incorporated the provider and the pharmacy into a technology solution which pushed gaps-in-care and messaging through the EMR and pharmacy system to drive coordinated solutions is the answer.
I don’t know when this will happen, but I don’t believe we’re going to put a dent in adherence until we think differently about this problem.