An average visit to the MD lasts less than 20 minutes and when you ask questions, you are interrupted in 18 seconds (see article).
Is this a fulfilling experience? I think they forgot to add the time you wait to get in the office and the lost opportunity cost for many of us (i.e., what else I could do with that time)?
“On the one hand, there are claims that doctors or drug companies are evil and dishonest. On the other hand, news reports describe triumphs of modern medicine in curing disease and improving quality and quantity of life,” says Dr. Brown in his new book, Navigating the Medical Maze: A Practical Guide. “How can so many seemingly intelligent, caring people reach such different conclusions? The solution is teaching people how to sort through conflicting advice so they can arrive at the best choices for themselves and for their families.”
I haven’t read the book yet, but I have a copy of it. I have a few things in front of it, but I did get this article from Dr. Brown that I thought I would post here.
Five Ways to Recognize the Best Doctors
By Steven Brown, M.D., PhD.
Doctors are just like any other group of people. Some are good, some are bad, and some are mediocre. How can you be sure you are getting one of the good ones? Rate your doctor in these five areas and see how he stacks up.
1. Thoroughness
The best doctors want to get your whole story. The first time she sees you, she (or her staff) should get your whole medical history, not just the details of the problem that brought you in that day. Since the parts of our bodies are all connected, problems in one part often relate to another part, even if the connection is not obvious to the layperson.
2. Communication
Does the doctor take time to listen to your story? Does he take time to explain the problem and answer your questions? Do you have to sit in front of the door to keep him from leaving? Doctors today are under considerable pressure. Costs of practice are rising, and payments from insurance companies are falling. Since doctors are paid based on how many patients they see, the only way to maintain their income is to see more patients in less time. If the doctor takes the time you need, that shows that he has decided to make less money in order to take better care of you. That is the kind of doctor you want.
3. Knowledge
Does your doctor know what she is talking about? When you ask why she is recommending one treatment over another, does her answer reflect knowledge of the medical literature? Is she threatened by questions, or does she welcome them? By the way, it is a good sign, not a bad one, if the doctor tells you she needs to look something up. That shows that she is humble enough and careful enough to check for the latest facts.
4. Self-sacrifice
If you need a doctor who does a lot at the hospital, such as a heart doctor, a lung doctor, or a surgeon, make friends with a nurse or secretary at the hospital. Ask them what doctors answer their pages quickly. Some doctors call back in less than a minute. Others take two hours to call back despite multiple pages. A doctor who cares about his patients will call back right away. He wants to know what is wrong, and he wants to do something about it. His patients are more important to him than his other activities. This exemplifies self-sacrifice. We all want a doctor who makes us a priority. If the doctor is in a specialty that does not go to the hospital, look for other evidence of self-sacrifice. Your friends may be able to tell you stories about a particular doctor who went the extra mile to help them.
5. Character
The single factor that ties these areas together is the doctor’s character. Anything you see that suggests poor character is a reason to go elsewhere. Has the doctor had any serious issues with your State’s Medical Board? You can find out by going to their web site. Does she treat her staff badly? Does he treat you and others with respect? If a doctor does not have good character, at some point it will affect his decisions. As vulnerable as we are to our doctors, we cannot afford that risk.
Anything that shows good character, for example doing well in the areas above, is a reason to overlook minor annoyances, such as an unpleasant receptionist. Having a doctor with good character is also more important than bedside manner. Some doctors may not seem particularly warm or friendly, but they exhibit the attributes we have discussed.
Fortunately, there are not a lot of truly bad doctors out there, but there are a lot who are mediocre. If your doctor does not show these traits, try to find one who does. If your doctor does show these traits, rest assured – he’s a keeper.
Dr. Brown is the author of Navigating the Medical Maze: A Practical Guide. He is a cardiologist in private practice, and is also a Clinical Associate Professor of Internal Medicine at Texas Tech University. He is a contributor to Chest, Circulation, and other health journals. For more information, please visit www.drstevenbrown.org.

 May 31, 2008
May 31, 2008 

 I get a lot of solicitations to talk about products on the blog. I also get a lot of general e-mails. The ones I generally respond to are people giving me a heads up about an article, press release, technology, or something else that I just wouldn’t have known about. That doesn’t mean I will do anything about it, but if I have time and find it interesting, I will usually click through the link. And, if it still catches my attention then I will write about it.
I get a lot of solicitations to talk about products on the blog. I also get a lot of general e-mails. The ones I generally respond to are people giving me a heads up about an article, press release, technology, or something else that I just wouldn’t have known about. That doesn’t mean I will do anything about it, but if I have time and find it interesting, I will usually click through the link. And, if it still catches my attention then I will write about it.
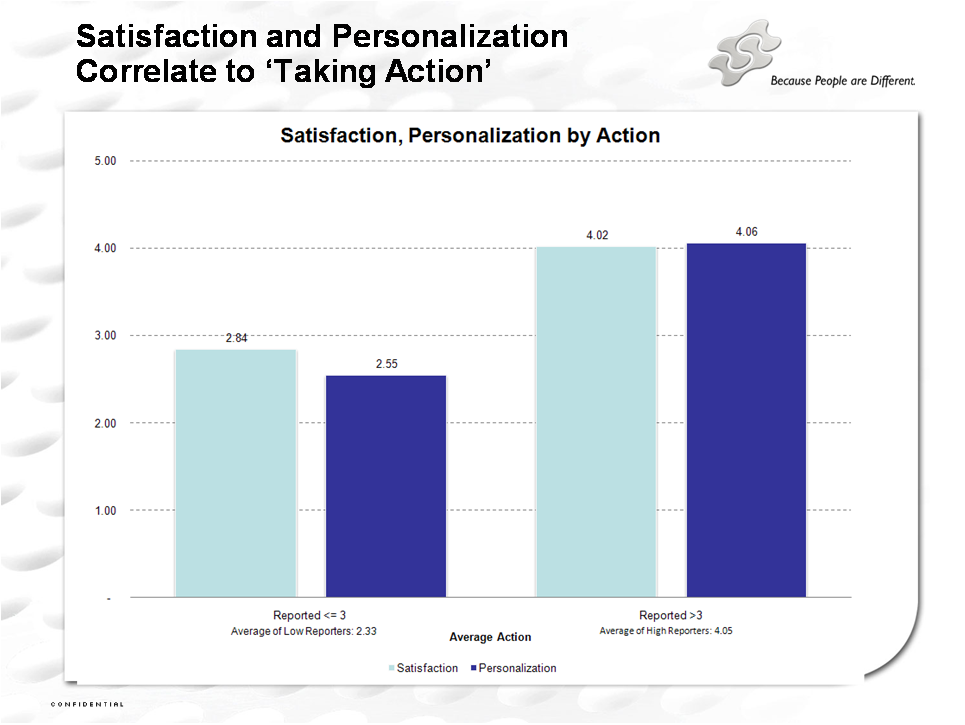
 I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.
I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.