January 31, 2008
January 31, 2008 
I was having an interesting discussion yesterday about how to solve a problem. The two opinions were whether there is a best answer or whether there are multiple best answers. It’s a great question.
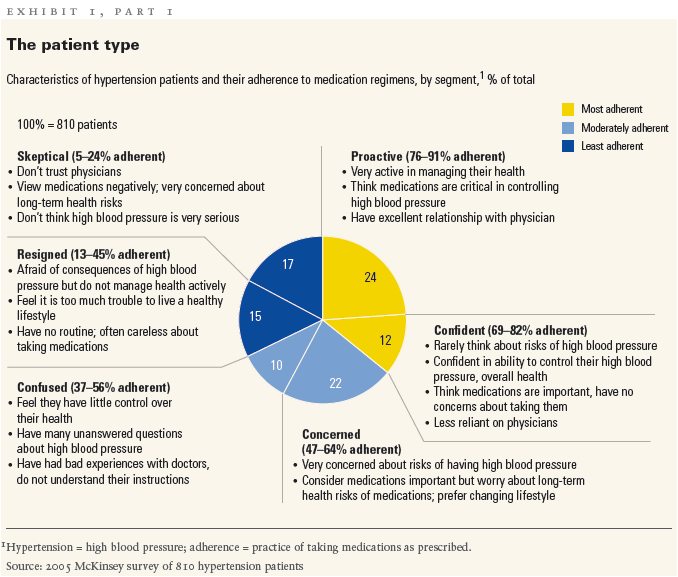
Let’s frame it this way. Is there a message that is most likely to drive compliance for a group? I gave them the benefit of the doubt that they aren’t crazy enough to suggest that one message works generally with no segmentation. (McKinsey‘s article “Getting Patients To Take Their Medication” has some good research around creating segments and showing how some of the segments vary in what they want.)
The other person was presenting a case that they could do lots of research on linguistics and other topics and suggest one optimal message that would work across broad segments of the population. I was of the opposite opinion that a personalized message that had certain core research but varied by geography, condition, age, income, benefit type, prior interactions, etc. was better. And, that what is good today may change both generally and individually over time.
I would rather get all the micro-niches of people to their highest compliance and adherence level versus getting a better average across all group.
Basically, my position is that there are multiple optimal solutions to the problem not just one. It triggered a memory for me of when I first went to business school. In architecture school, design is somewhat subjective. (There are some logical rules such as the Fibonacci Sequence which serve as guiding principles of scale…for example.) We were taught to always bring three solutions to our initial presentations to let the judges decide which one we should push to finalize. We had to pick one for a deliverable, but it was always a tradeoff. In business school and the hard sciences, there is often only one answer that is valid. (1+1 always equals 2.)
But, for communications, marketing, and other things, it seems obvious to me that companies are best served by dynamic flexibility that allows them to bring multiple solutions to the market in parallel that adapt to different patients and change over time to respond to the market and the patient.
Here is a quick snapshot of the segmentation from the McKinsey report…