June 20, 2013
June 20, 2013 
The AMA has opened an interesting discussion in the past few days with their decision to recognize obesity as a disease. On the one hand, we all know obesity is a problem that’s impacting our overall health and productivity across the world. On the flip side, will this actually change anything?
Key discussion points:
- What is a disease?
- Is BMI a good metric to use? If not, what should be used to measure obesity – waist?
- How do you treat it?
Here’s a few quotes from some articles:
“Right now, physicians will treat high blood pressure, diabetes, give patients medications and say, ‘Oh you also need to lose weight,’” Khaitan told FoxNews.com. “I think (this) gives the physicians a little more credibility in pushing patients to address obesity and become healthier. It’s recognized as a disease…not just something that (because) you have poor lifestyle habits, this is your problem.” (Fox News)
Obesity is not just a health risk but a disease. Estimates of the genetic contribution to weight gain in susceptible families range from 25—40% with a greater heritability for abdominal fat distribution of 50%1>2. Obviously there is a major environmental effect but this genetic susceptibility alone removes this condition from a social stigma to the disease category. (British Medical Bulletin 1997)
“The American Medical Association’s recognition that obesity is a disease carries a lot of clout,” says Samuel Klein, director of the Center for Human Nutrition at Washington University School of Medicine in St. Louis. “The most important aspect of the AMA decision is that the AMA is a respected representative of American medicine. Their opinion can influence policy makers who are in a position to do more to support interventions and research to prevent and treat obesity.” (USA Today)
Telling all obese people that they have a disease could end up reducing their sense of control over their ability to change their diet and exercise patterns. As experience with addictions has shown, giving people the sense that they suffer from a disease that is out of their control can become self-defeating. So the disease label should be used sparingly: just as not all drinking is alcoholism, not all overeating is pathological. (Time)
Here’s a few facts from the Obesity Action Coalition:
- In the United States, it is estimated that 93 million Americans are affected by obesity.
- Individuals affected by obesity are at a higher risk for impaired mobility and experience a negative social stigma commonly associated with obesity.
- Socioeconomic status plays a significant role in obesity. Low-income minority populations tend to experience obesity at higher rate and are more likely to be overweight.
- In 2001, the states with the top five percentages for obesity were Mississippi, West Virginia, Michigan, Kentucky and Indiana.
- Almost 112,000 annual deaths are attributable to obesity.
- In the United States, 40 percent of adults do not participate in any leisure-time physical activity.
Here’s also a few things you might not realize about obesity from Yale:
- Finding 1: Obesity can raise some cancer risks
- Finding 2: Obesity is tied to heart attacks in younger adults
- Finding 3: Obesity can ruin your day
- Finding 4: Obesity speeds up girls’ puberty
- Finding 5: Obesity is a cause of diabetes in kids
- Finding 6: Obesity in middle age increases risk for dementia
Let me give my hypotheses on why this might matter:
- In theory, this is supposed to increase the likelihood that physician’s talk about obesity with their patients. This would be great, but I think most research shows physician’s aren’t prepared or comfortable with this discussion. Will the fact that it’s a disease make this easier? Maybe.
- This may be a boon for the obesity Rx market (assuming any of them work and have minimal side effects). Physician’s may be much more likely to write an Rx for a disease than a lifestyle issue.
- This may help get obesity Rxs and bariatric surgery to be covered by health insurance. The downside of this is that more people may not actually change behavior (diet, exercise, sleep) but instead look for a “quick” fix through drugs and surgery.
In my mind, there is a best case scenario here:
- Calling it a disease drives awareness among the healthcare community.
- This increases investment in resources to treat obesity.
- Treatment is viewed more like mental health to include drugs and behavioral therapy.
- Physician’s get trained on the disease.
- Pharma details physicians on the disease and creates CME programs.
- Patients start to take this more seriously.
- Plans cover obesity – insurers, employers, CMS.
- Obesity becomes a broad program including diet, exercise, coaching, Rx, and bariatric surgery following a progressive approach to treatment tied to your starting point.
- Companies link incentives to managing weight.
- New metrics are designed that are better than obesity.
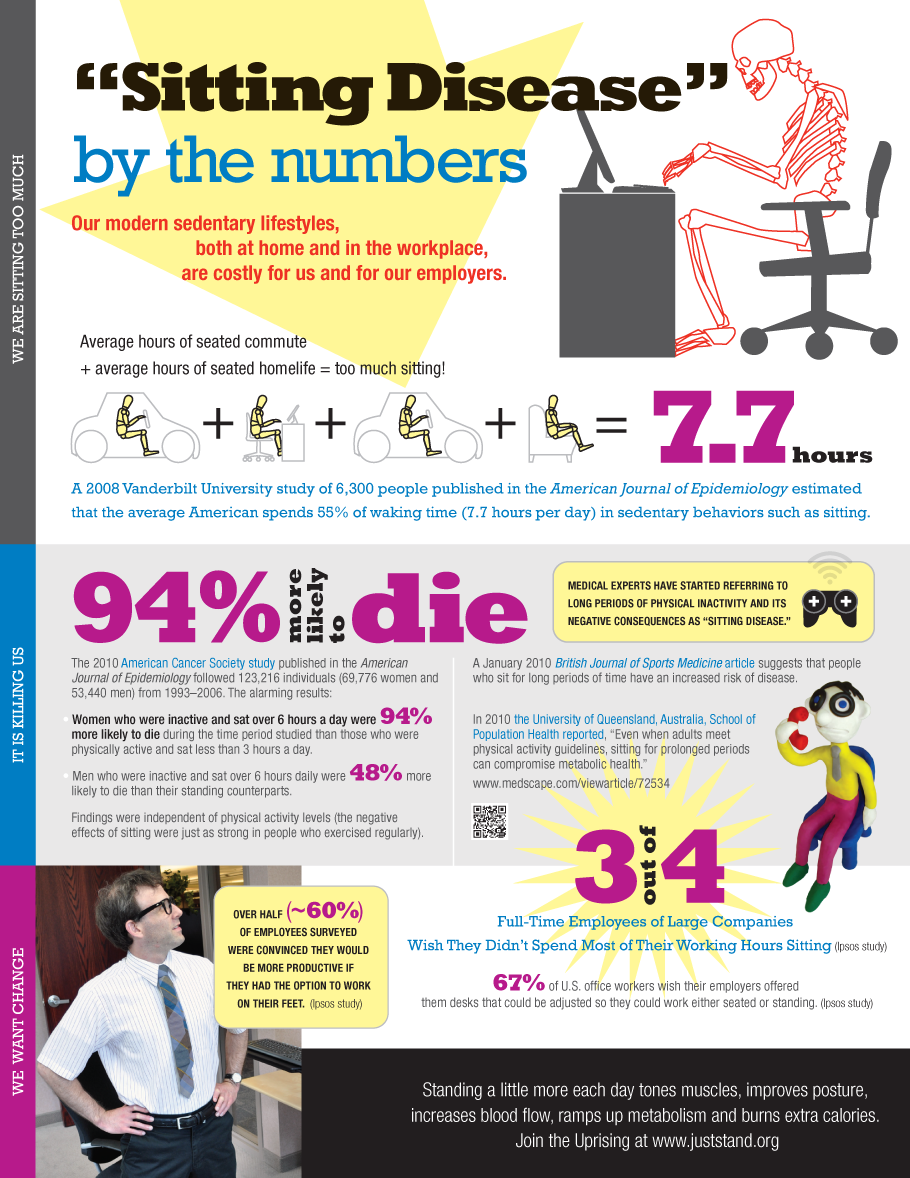
Of course, one of the more recent articles which was depressing on this topic was that exercising regularly may not overcome the impact of sitting the rest of the day. That makes it very hard to increase caloric burn while having a job that requires lots of desk, computer, and meeting time.