
 November 30, 2007
November 30, 2007 
 The AHIP magazine Coverage (Sep + Oct 2007) also has an article about retail clinics. There were a few takeaways here:
The AHIP magazine Coverage (Sep + Oct 2007) also has an article about retail clinics. There were a few takeaways here:
- Someone is finally going to try and offer an airport based clinic (AeroClinic). This seems to make sense as some airports are basically shopping malls in disguise.
- 5% of consumers know about retail clinics and have used them. Maybe I am too close to the space, but it seems like this is all I hear about.
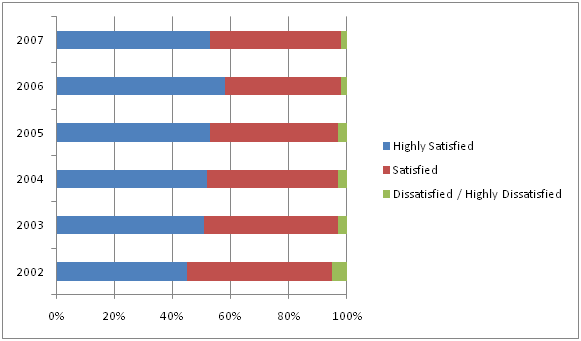
- 90% of consumers say they are satisfied with the quality of care…85% with the quality of staff…83% with the convenience. [Harris Interactive survey of 2,441 adults in March 2007 for the WSJ]
- 42% of those that visited clinics were covered by insurance for some or all of the services provided.
- Co-pays ranged from $15-$35.
- 22% of those that visited clinics were uninsured. (which is a little more than the % of the general population that is uninsured – if my back of the envelope math is right)
- The forecasted growth of clinics – 700 (2007); 1,500 (2008); 4,000 (2010). I am a little skeptical here, but I wouldn’t think you could have 3 Starbucks at one intersection or 6 pharmacies within a 3 mile stretch of one street. (both real examples)
- There are some challenges around the model including from the AMA (American Medical Association) around conflicts of interest (i.e., clinics being owned by pharmacy chains) or the erosion of the “medical home” for the patient. Ultimately, there should be some health outcomes metric which is used – better compliance, more prevention, lower cost per disease state, etc.
- BCBSMN found that members who were part of a consumer directed healthplan were twice as likely to use a retail clinic. They have been very closely involved with MinuteClinic from the beginning.
- An individual from HealthPartners raises an interesting risk around provider capacity pointing out that if use of retail clinics increases provider capacity then it might actually increase total healthcare costs for the system. I guess this implies that the physician or hospital could charge more if they weren’t as busy. Not sure I buy the logic, but my micro-economics could be off.
Several groups have come out with standards or guidelines including:
- The American Academy of Family Physicians (AAFP) has their Desired Attributes of Retail Health Clinics
- The American Medical Association (AMA) has a policy on “Store-Based Health Clinics“
- The Convenient Care Association has its standards
- And MinuteClinic has actually chosen to get accredited by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) which means that it complies with more than 180 nation standards and 500 performance measures

 When I got my
When I got my 





{kind=link}
{kind=link}