March 24, 2014
March 24, 2014 
You’ll hear this buzzword – “beyond the pill” – come up every once in a while in a discussion with a pharmaceutical manufacturer. As the drug pipeline has dried up and generics have become the norm for oral solid medications, the question is how do these behemoth companies “pivot” to leverage their massive global footprints, their feet on the street, their deep disease specific insights, and their medications.
“In population health, what once drove revenue becomes a source of cost. If products, services, and therapeutics don’t lower costs, meaningfully improve outcomes, and help better patient experience, population health managers simply won’t use them.” Jerry Cacciotti, Partner, Health & Life Sciences, Oliver Wyman (source)
I’m a big believer in this strategy. Imagine what they could do in terms of services to wrap around obesity drugs. Imagine how they could support patients with diabetes or with cancer. While the short-term view is that these actions might help differentiate them from a formulary or specialty pharmacy perspective, I would argue that they might actually come out with new business models like Merck is doing with Vree Health.
Ultimately, it all begins with an understanding of several issues from the outside-in:
- What is the patient journey?
- How do they experience the healthcare system? (e.g., clinics, MDs, pharmacists, family)
- How or what influences their experience? (e.g., Dr. Google)
- How do their experiences change over time? (e.g., newly diagnosed versus chronically sick)
- Which experiences do they remember? (or as one of my clients call it – the Golden Moments)
- What does the patient really want or need? (think about Maslow’s hierarchy of needs)
- Where is the patient (especially from a digital perspective)?
- What are the patient’s expectations for you (pharma) or another entity?
- How do they feel about you?
- Do they trust you?
- How do the other constituents in the care team interact with you? With the patient?
- How do you create a culture of empowerment, consumer focus, and transparency to really understand the needs of different constituents, react to them internally, and embrace issues dynamically?
In this consumer experience space, I often look to Bruce Temkin’s work and research. He does a great job at a cross-industry perspective. In healthcare, I’ve been very motivated by the work of Ingrid Lindbergh who was at Cigna and then moved to Prime Therapeutics. She’s my role model for what I want to do in a large healthcare company.
Two things got me thinking about this topic. First, I was struck this weekend that there was research showing that people who struggle to buy food for their families are non-adherent. I really hope that anyone in this field wasn’t surprised by that fact. Of course, the struggle is that everyone working in the field is often constrained by their view of the world which often doesn’t include much experience with poverty.
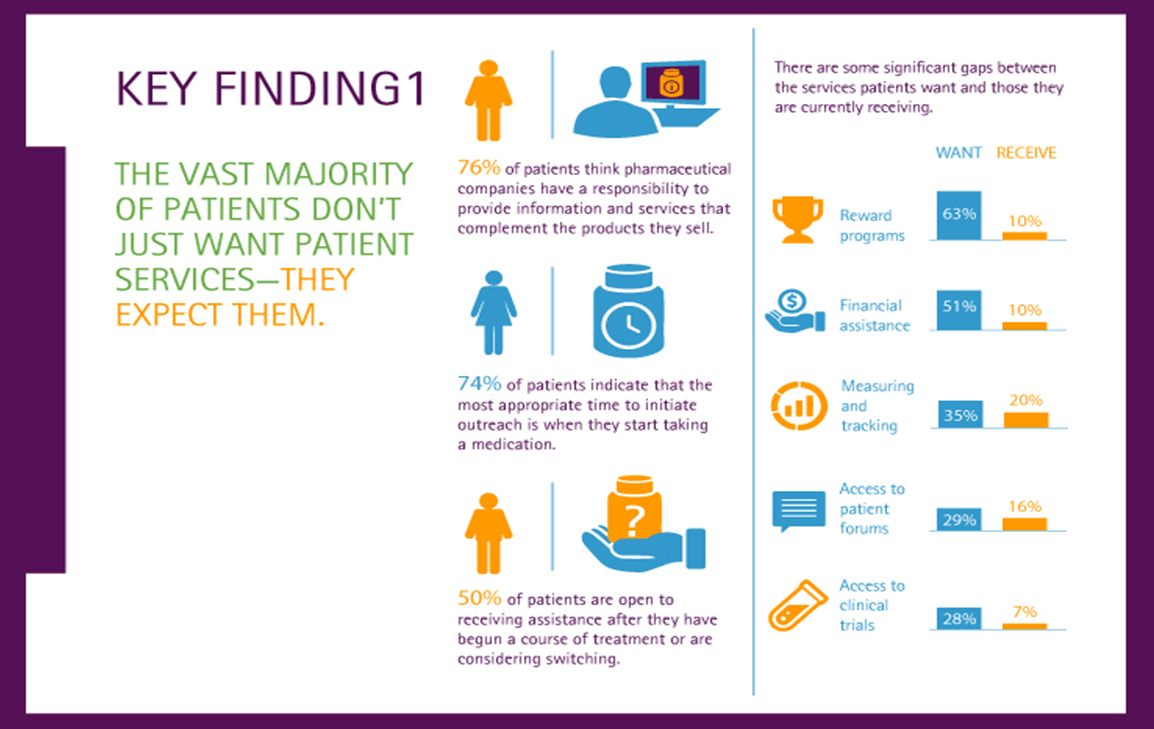
Second, I was sent a new research piece by Accenture called “Great Expectations: Why Pharma Companies Can’t Ignore Patient Services”. It made me think about Dennis Urbaniak’s move from Sanofi where he was leading a lot of innovation to a Managing Director at Accenture. Perhaps, he will bring some of this type of innovative thinking to more pharma companies.
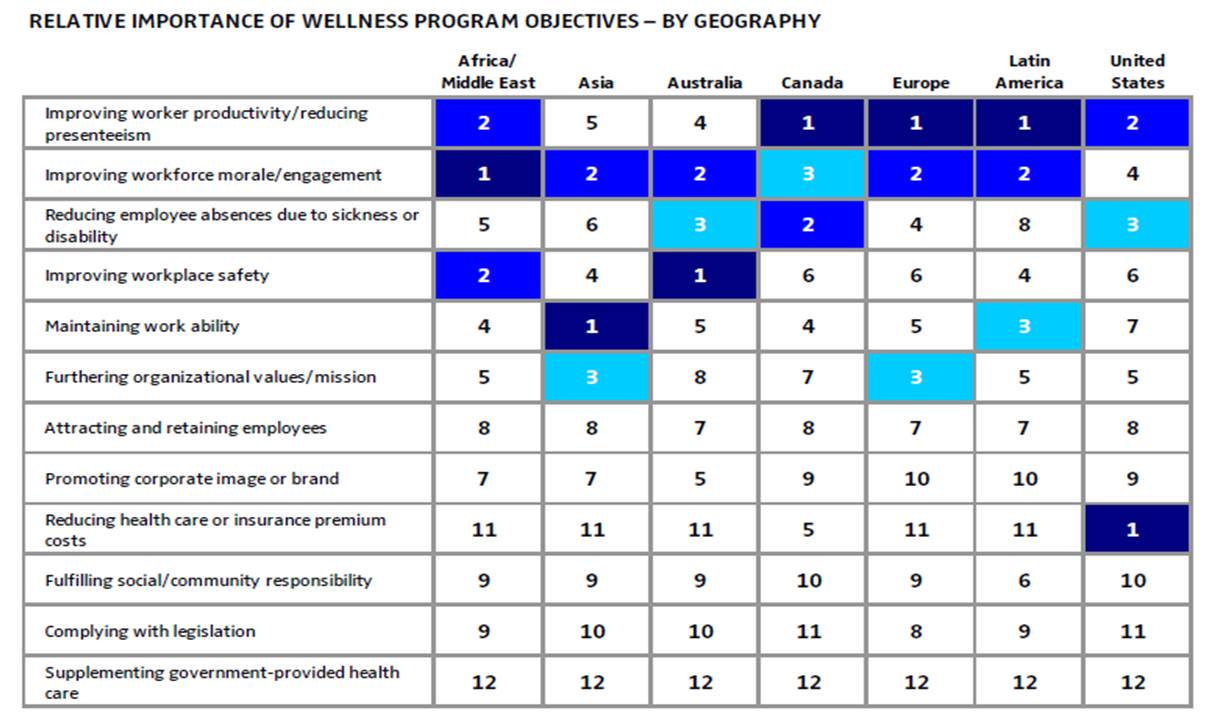
Here’s two infographics from the Accenture report which I think help hammer home the point of why beyond the pill is necessary: