November 30, 2010
November 30, 2010 
It’s always nice when you get on the marketing distribution list from companies. I love to get the PR and marketing materials to review. Medco recently sent me this document called “9 Leading Trends in Rx Plan Management: Findings from a National Peer Study“.
The survey was across 380 organizations plus 100 consultants and brokers. And, the survey was conducted prior to health reform passing so that’s an important timeline to keep in mind. It’s a nice quick read with lots of stats and charts from the survey with comparisons to last year’s numbers.
Executive Summary:
- Less than 40% said they were extremely or very concerned about economic conditions affecting their ability to offer the same level of prescription benefits over the next 2-3 years. (down from 60%)
-
Plan sponsors are increasingly eager to find cost control solutions:
- 90% – promoting the use of formulary products (brand and generic)
- 80% – encouraging the use of mail order
- 83% – helping members make more effective healthcare choices
- 76% of plan sponsors state that balancing costs with care is the key philosophy (which is a reversal from 5 years ago where it was providing broad coverage)
- Respondents see pharmacy as representing 22% of their overall costs (a higher number than I’ve seen before so I’d like to see actual data here)
- Surprisingly, plan sponsors were more concerned over DTC advertising and minimal attention to personal health than aging and use of specialty drugs
- 72% EXPECT their PBM to help reduce overall healthcare costs (what I’ve been saying for a few years)
- 79% say that specialty pharmacy is better managed by the PBM than the health plan
The 9 leading trends:
- A transformative shift in benefit philosophy continues
- Rising costs replace economic woes as key affordability issue
- Plan sponsors prefer targeted but limited government employment
- Use of integrated data is becoming standard practice
- CDH plans are struggling to gain momentum
- Specialty medication management programs are increasing sharply
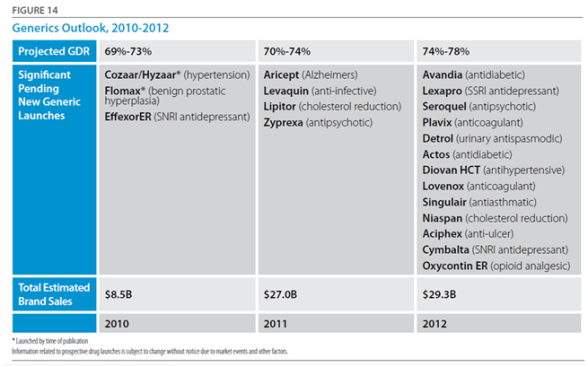
- Generics and preferred drug programs moving from incentives to mandates
- Decisive move towards stronger mail incentive programs
- Plan sponsors look to PBMs to reduce overall healthcare costs
(The ones that surprised me here were #4 which I just haven’t seen significant movement on and #7 where I haven’t seen much in the way of mandates, but I’m on the outside looking in these days.)
#1: Transformative Shift in Benefit Philosophy
- Only 6% are focused on limiting coverage
- Honoring retiree commitments is still the #1 factor in guiding retiree benefits
- 95% of benefit advisors agree
#2: Rising Costs as Key Affordability Issue
- 72% blame physicians for complying with patient requests for more expensive branded medications
- 52% believe that engaging members to make better health and cost related decisions is their number one priority (which is exactly what Silverlink does for clients!)
- 95% of benefit advisors agree
#3: Targeted but Limited Government Involvement
- 60% say the government should have minimal or no role in providing prescription benefits (only 15% preferred a private plan)
- 71% want the government to help bring generic biologics to market faster
- 42% believe the government should mandate e-prescribing initiatives
- 75% of benefit advisors agree that government proposals will help lower Medicare Part D costs
#4: Use of Integrated Data
-
64% use integrated data to improve health and financial outcomes (I would guess much of that is outsourced to 3rd parties. This also still doesn’t include lab values.)
- 74% do it to improve case management
- 70% do it for disease management
- 68% do it to identify members at risk
- 95% of benefit advisors agree on the likelihood of recommending data integration over the next 2 years to control drug costs
#5: CDH Plans are Struggling
- 27% of respondents offer a consumer-directed health plan but 73% say their members are reluctant to join
- It was virtual tie between those that thought CDH plans helped reduce Rx costs and those that didn’t…but the majority of people agreed that they help employees better understand the real costs of healthcare
- 67% of benefit advisors agree on the likelihood of recommending a CDH plan over the next 2 years to help control costs (which seems out of line with the employer perspective)
#6: Specialty Medication Management Programs are Increasing
- 83% of respondents plan to install clinical and cost-management programs to help contain the cost of specialty medications
- 40% cite specialty as the key cost driver
-
Respondents believe that billing under the pharmacy benefit:
- Provides more consistent pricing (79%)
- Provides a better understanding of therapy management savings opportunities (77%)
- Provides a more complete and accurate picture of specialty spending (80%)
-
The programs being used are:
- Utilization management (64%)
- Limit days supply (63%)
- Preferred pharmacies (58%)
- Step therapy (55%)
- Move coverage from medical to pharmacy (41%)
- Waive copayments to increase use of a preferred pharmacy (9%)
- 76% of benefit advisors agree on the impact of UM programs controlling specialty drug costs
#7: Mandates Over Incentives For Formulary Agents
- 58% are requiring the use of generics and preferred drugs (does this mean going back to closed formularies?)
- 90% use programs that incent (i.e., lower copays I assume)
- 94% are likely to increase member communications to encourage the use of generics
- 63% of benefit advisors agree on mandating the use of generics to control costs
#8: Stronger Mail Incentive Programs
- 58% have installed programs where the member pays more at retail after a set number of refills (I think this is a Medco anomaly…they’ve always had the highest mail utilization)
- 85% have a cost-share strategy that favors mail
- 38% waive one or more copays as an incentive to move to mail
- 5% auto-enroll members in mail
- 54% believe dispensing errors are less likely at mail (while 7% believe retail is better)
- Mail order is seen as having a better chance to maximize generic use (by a 5:1 margin over retail)
- 69% of benefit advisors agree that dispensing errors are less likely at mail than retail
#9: PBMs and Overall Healthcare Costs
-
Why use a PBM:
- More focused and experienced at controlling drug costs (88%)
- Most competitive drug prices (88%)
- Provide detailed analysis and reporting to help explain cost drivers and identify savings opportunities (87%)
- More innovative approaches to controlling costs (83%)
-
After cost control of Rx, what do they look for in a PBM:
- More effective in promoting adherence (69%)
- Helps control overall healthcare costs (72%)
- Better medication counseling (70%)
-
Benefit advisors believe the following are the most critical priorities for plan sponsors:
- Engaging members (39%)
- Controlling specialty costs (24%)
- Ensure the pharmacy benefit supports a broader health strategy (20%)