
This is a nice infographic on some of the ACO activity around the country.

 December 31, 2012
December 31, 2012  0 Comments
0 Comments
This is a nice infographic on some of the ACO activity around the country.
December 30, 2012 0 Comments

Are you going to this year’s conference (February 18-20th) in Las Vegas? I’ll be presenting again this year, and I hope to see some of you there. If you’ll be there, let me know and we can connect.
This year, I’m going to talk about one of my favorite topics which is how the pharmacy industry needs to transform itself. This touches on several topics which I’ve blogged about multiple times:
Do you have a specific example of how you see companies (pharma manufacturers, PBMs, or pharmacies) transforming from a traditional Fee-For-Service (FFS) model to an outcomes based model in terms of payment and how that is changing the way they do business? I’m always interested in learning more.
Here’s the official description from the brochure for the conference.
Pharmacy — Data, COEs, Predictive Models, and Consumer Engagement
George Van Antwerp, Vice President, Product Development, inVentiv Medical Management
ACPE UAN 0221-9999-13-009-L04-P 1.0 Knowledge-based contact hour
Pharmacy is the most used benefit, and for most chronically ill patients, they take multiple medications per day and interact with their pharmacist/pharmacy frequently. With the transformation in healthcare to an outcomes-based focus, PBMs, pharmacies, and pharma are looking at new models and new ways to work with payers, providers, and patients to be part of the care team. We will explore how companies are using this data and technology to intervene, change behavior, and improve outcomes from a broader population health management perspective.
December 29, 2012 1 Comment
This is an infographic on an interesting program out of USC which received money from the CMS innovation fund.

December 28, 2012 1 Comment

Do you know your Klout score? I know mine – 51. Is that good or bad? I guess it’s all relative. Mine is only based on Twitter and LinkedIn.
The bigger question is should I care. I’ve struggled with why to care, but it finally hit me the other day. There are a few circumstances where I might care:
As an average person working for a company, I’m not sure it matters. Of course, you can argue with the “scoring” process, but the reality is that people do want some benchmark to compare themselves to for what they do online. The interesting question is whether companies will care. And, is there a minimum that you should have just to be able to say you understand and use social media?
Here’s a few recent articles discussing the topic of Klout.
It’s competitors are Kred and PeerIndex which I only went to because of this post. But, I signed up for them to see what my scores where there.


My question would be how do you adjust this for people (like me) who don’t use Facebook or should that fact alone exclude me from certain things like being a community manager for a product that needs a Facebook presence? Perhaps.
So, if you’re hiring a mHealth or social media team, you might want to know their Klout (or Kred or PeerIndex) scores (on average for the team). I’d say it’s like gamification. I wouldn’t want someone just using that buzzword with me. I’d want to know the last game they got sucked in to. Why it kept their attention? And, then I’d ask them things like why they think Steam is gathering gaming apps in their and whether it’s critical path for them in gamifying their app.
December 27, 2012 0 Comments
Home Health Aides: the Unsung Heroes of Healthcare
It takes a special type of person to succeed in the field of home care. Home health aides’ commitment to their patients really does make them the unsung heroes of the healthcare field. Often times, after patients are discharged, they recall the names of their home health aides and write them letters of gratitude.
Home health aides assist patients during very vulnerable times. Hospice home health aides, for example, provide comfort to patients near the ends of their lives.
A home health aide is sometimes the only person a patient sees on a given day. Therefore, aides go beyond providing much needed medical help; they also provide compassion and an emotional connection. They might be the only person to whom a patient expresses their emotions and thoughts. They’re typically a patient’s housekeeper, caretaker, and compassionate listener.
These compassionate care givers work on the front lines of healthcare to assist seniors, people with disabilities, people recovering from illnesses, and others unable to take care of themselves. Home health aides help their clients with daily activities such as grooming, hygiene, and eating. They give clients their medication and also perform tasks such as dressing wounds, changing bandages, and applying topical medications.
Home health aides also clean their client’s home, do their laundry, and changes their linens. They plan nutritious meals and shop for and prepare the food. They also run errands for their clients and provide much needed time off for family caregivers.
Testimonials
Here are a few excerpts from letters written by actual patients in which they express their thanks for their home health aides:
“Just a note to thank you for the time you spent with my sister and me. You were very helpful and your sensitive manner put us at ease so that we could understand and deal with mother better at such an emotional time. You folks who work with ill people are very special and I for one thank you for being that way.”
“I want to thank you for sending Dolores as my homemaker. She does a great job; she sees what needs to be done and does it! This is so helpful to me. She’s very pleasant to have around.”
“Thank you so much for your promptness in responding to my need. I must say, Ellen was excellent. She was so warm and kind. I responded favorably to her at once. She worked hard and seemed to fit my rhythm so well. I had been quite shocked by my recent experience and was feeling quite low. Her spirit and enthusiasm had such a positive effect on me. I think she is a gem and I am so grateful to have had her come into my life and care for me.”
(Source: Metropolitan Home Health Services, Inc.)
Home health aides make a huge difference in the lives of their patients and their family members. However, according to the Bureau of Labor Statistics, the median annual salary of home health aides is only $20,610. It’s no question that these unsung heroes who play a vital role in improving the quality of life of their patients deserve a whole lot more!
Brian Jenkins writes about the home health aide career field, as well as other careers in allied health, for the Riley Guide.
December 27, 2012 1 Comment
Medical Technological Innovations in Our Future
The history of medicine is full of technological innovations. The ECG in 1913, the Band-Aid in 1920, the cardiac pacemaker in 1950, CAT scans in the 1970s and the completion of the Human Genome Project on 2003 are just a few of the many inventions in just the last century.
Yet, we are now standing at a threshold of medical technological change unparalleled in history. In the next 20 years of the Shift Age, there will be more technological change than in the last 100 years. Let’s take a look, in loose chronological order at these changes of the future.
Low Cost Personal Genetic Mapping
In 2013 we will be able to have most, if not all, of our personal genetic maps completed for under $1,500, an outgrowth of the Human Genome Project. This is very significant as the knowledge each of us will learn from our individual genetic maps can help us act in a preventative manner. If, for example you are in your twenties and you find out that you have a genetic disposition to early onset Alzheimer’s, you can spend the next few decades doing whatever current medical wisdom says might slow the onset of Alzheimer’s; taking Omega-3 fish oil, working out every day and other discoveries about the disease. In other words, personal genetic maps will allow us to address whatever genetic dispositions we might have, BEFORE they happen to us!
Bionics
There are incredible developments in the area of bionics and replacement “parts” for the human body. New artificial arms and legs can now be controlled by thought and brain-waves. These are now being tested on veterans of the Iraq and Afghanistan wars. In the next few years there will be replacement eye-balls that will provide 20/20 vision for years. There will be ear implants allowing deaf people or people who have lost a significant part of their hearing to hear clearly again or for the first time. In the next decade we will develop replacement parts that are better than the “parts” we were born with!
Tissue Regeneration
Recent breakthroughs in stem cell research are pointing the way towards tissue regeneration for all of us. In the years ahead we will be able regenerate organs. This will lead us to each have the opportunity to regenerate organs from our own tissue, eliminating both the need for an organ donor and the possible rejection of the new organ that often happens. This will not be inexpensive, but it will be possible in the next decade.
DNA Pharmaceuticals
The technology for the development of DNA Pharmaceuticals flows from the ability to map individual’s genetic maps. Think of them as personalized drugs. We are all familiar with the “lowest common denominator” drugs as we see them advertised all the time. This great pill will lower your blood pressure, but it might also cause sudden death syndrome, erectile dysfunction, or loss of sight. With ever more precise genetic information, drugs in the future will be personalized to each patient, eliminating these horrible side-effects. What works for one person will not work for another and this reality will be finally addressed in pharmaceuticals.
Nanotechnology
A nanometer is a billionth of a meter. A human hair has a diameter of approximately 50,000 nanometers. Medical science is currently creating microscopic bots that can enter and move freely within the human body. The early use of this technology will be to directly attack cancers in the body with transported DNA-customized chemicals. Nanotechnology will allow us the ability to precisely deal with such cancers and not degrade the entire body with chemotherapy
Human Cloning
In the last two decades animals have been successfully cloned. This history, combined with some of the breakthroughs listed above, make the possibility of human cloning a reality by 2020, if not before. The real questions here are of course moral. What to do with experiments gone wrong? How to treat experiments gone right? The history of human and religious morality will be confronted with this real possibility. It will be able to be done, but will we want it done?
Guest Post written by:
David Houle is a futurist and author of the highly regarded blog Evolution Shift. He is the author of The Shift Age and The New Health Age, and a contributor to O The Oprah Magazine, The Huffington Post,and NPR. Houle spent more than 20 years in entertainment, as part of the executive team that launched MTV, Nickelodeon, VH1 and CNN Headline News. A sought-after lecturer, he was recognized as Speaker of the Year from Vistage International, the leading global organization of CEOs. Houle is Futurist in Residence at the Ringling College of Art + Design in Sarasota, Florida.
December 26, 2012 0 Comments
I found this infographic here – http://www.hitconsultant.net/2012/07/25/how-patients-learn-in-the-digital-age-infographic/.

December 26, 2012 2 Comments
The short answer is that a PBM is the company hired by your employer (either directly or through your health insurance company) to manage your pharmacy benefits. When you use your pharmacy card at the retail pharmacy to get a prescription, the pharmacy interacts with your PBM electronically to find out if the drug is covered and the copay to you the consumer.
*****************
Back when I first started blogging, I used a lot of my experiences at Express Scripts to shape some of my perspectives about the PBM or Pharmacy Benefit Manager industry. It took me a few months before I realized that some people reading the blog didn’t know what a PBM was. That led me to my all time most popular blog post – “What Is A PBM?”
Since that was over 5 years ago, I figured it was time for an update.
The market has shifted in the past 5 years especially with Express Scripts purchase of Medco to become the largest player in this space. Walgreens has also divested their PBM to CatalystRx which was then bought by SXC and the new entity renamed CatamaranRx. At the same time, you’ve seen United Healthcare insource their PBM business from Medco to combine it with their old Pacificare PBM to create OptumRx. You’ve also seen Humana’s PBM business and mail order business – RightSourceRx – grow significantly.
There are other big PBMs which I didn’t mention such as CVS Caremark which after years of rumors about them splitting back up seems to have proven their case as an integrated, retail-owned PBM. There is MedImpact which has 32M lives according to the latest PBMI market share report, and Prime Therapeutics which is a PBM owned by several of the BCBS plans. Additionally, Aetna, Cigna, and several other managed care companies also have their own PBMs.
While I would have argued that the PBM wasn’t typically known to consumers 5 years ago, I think that the very public dispute between Walgreens and Express Scripts has changed some of this.
But, what a PBM does is relatively simple:
The PBM’s clients are employers who are self-insured, government entities (i.e., state employees, Department of Defense), unions, TPAs (third party administrators), and managed care companies (i.e., BCBS of).
PBMs are sometimes referred to as middlemen, but I will point to a few other posts on this:
In general, if you’re looking for more information on PBMs, I would point you to several sources:
The only other blogger who really offers any coverage of this space is Adam Fein which his blog – Drug Channels.
December 26, 2012 0 Comments
Mobile Health (“mHealth”), the use of mobile technology to deliver healthcare services and information, skyrocketed in 2012. 44 million health apps will have been downloaded by the end of the year (predicted to reach 142 million downloads by 2016), and consumers are now spending $700 million per year on these apps. There are over 10,000 health apps in the iTunes app store, the number of American using smartphones for health information grew from 61 million to 75 million this year, and 88% of doctors would like patients to monitor their health at home.
So what are some of the top medical and health apps we’ll be using in 2013?
1) MediSafe Project – MediSafe Project is the first-ever cloud-synced pillbox app that not only reminds you when it’s time to take your medication, but also sends your family, friends and caretakers alerts if you miss a dose, leveraging the power of your support system to keep you healthier. Compatible with the FDA’s drug database, generic and brand name medications autocomplete as users enter them – automatically recording the correct pharmaceutical name, manufacturer and medication strength. Or, use your smartphone’s camera to snap the FDA’s universal National Drug Code (NDC) number, found on all original pharmaceutical packaging, to enter a medication. iPhone and Android. Free.
2) EveryoneEat! – EveryoneEat! helps the 150 million American living with a chronic condition or dietary restriction find restaurants serving meals appropriate for them. By partnering with nationally recognized health associations, clinical and registered dietitians, and thousands of your favorite restaurants, the app finds dishes that meet your dietary needs and displays them by cuisine type or restaurant name. Simply enter your age, height, weight, gender and activity level, and the app is ready to use. iPhone and Android. Free.
3) WebMD Pain Coach – WebMD Pain Coach helps people with chronic pain conditions make daily health and wellness choices, so they can manage their pain smarter. From back pain to migraines, the app lets you record daily pain levels, export your pain history to PDF and email it to your doctor. You can also select doctor-approved goals from five lifestyle categories related to your pain condition(s): Food, Rest, Exercise, Mood, and Treatments, view ‘bite-sized’ tips matched with your goals and organized into the same five lifestyle categories, and read hundreds of articles, videos, slideshows and quizzes on pain management related to your condition(s). iPhone only. Free.
4) Emotion Select – Part of the ‘Spotlight Autism’ app series, Emotion Select helps children on the Autism Spectrum Disorder (ASD) or those suffering other social delays practice learning and identifying emotions. After reviewing illustrations for joy, sadness, anger, surprise, and fear, children are given the chance to anticipate and apply them in ‘real life’ social situations. Includes statistical analysis for parents, teachers and therapists to track specific strengths and weaknesses of children’s learning progression. iPhone only. $9.99.
5) Emergency Kit – Emergency Kit is an easy way to aggregate all of your most critical information – and could save your life in a medical emergency. Emergency technicians will be able to view your vital stats including blood type, allergies, medications, and emergency contacts within the app. It can also turn your phone into an SOS light beacon, send out an emergency text message or email with your GPS coordinates, or look up how to treat different injuries. Windows Phone. Free.
This post was written by:
Omri ‘Bob’ Shor is co-founder and CEO of the MediSafe Project, the first cloud-synced mobile app helping families prevent emergencies caused by over- or under-dosing medications.
Inspired to create the MediSafe Project with his brother after their diabetic father accidentally double-dosed on insulin, Shor drew on his considerable entrepreneurship experience to successfully develop and bring the product to market in less than one year. MediSafe continues to receive support from the Microsoft Accelerator for Windows Azure, after graduating its inaugural program for early stage, mobile & cloud-based startups.
Previously, Shor served as marketing and product manager for legal app developer Masadit Software, where he increased the company’s roster from eight to 2,000 clients, enabling it to reach sustainable profitability. Prior to that, he managed a department of twenty-five salespeople for Yedioth Ahronoth, Israel’s most widely circulated newspaper.
Since 2012, Shor has been a leader of Entrepreneurs in Jeans, a Boston-sponsored organization promoting the entrepreneurial scene in his hometown of Haifa, Israel. He was also an Israeli Air Force Flight Academy cadet and decorated army sergeant, having commanded a paratroopers’ unit in the Israel Defense Forces from 1999-2002.
Shor received an MBA in Entrepreneurship & Strategy, cum laude, from The College of Management – Academic Studies (COMAS) in Rishon LeZion, Israel. He lives in Haifa with his wife and daughter.
December 23, 2012 1 Comment

As I think about our healthcare system, there are lots of things I’d like that would be useful in improving patient outcomes. So, beyond the obvious things that we’d all like such as:
Here’s what’s at the top of my list from a technology perspective.
On a related note, I’d love to find a technology that allowed me to take all my blog posts and tweets and configure them by topic into an e-book. That seems like something logical.
December 21, 2012 0 Comments
As part of a new study mentioned on The Doctor Weighs In, it shows that physicians spend an average of 10 minutes and 10 seconds with patients in an average visit. Of that, 99 seconds (or 16% of the time) they are discussion prescriptions. The big question is what are they discussing.

A 2006 study showed the following:
74 percent of the doctors mentioned the trade or generic name of the medicine, and 87 percent stated its purpose. Sixty-six percent said nothing about how long to take the medicine, 45 percent did not say what dosage to take and 42 percent failed to mention the timing or frequency of doses. Physicians mentioned adverse side effects only 35 percent of the time.
Of course, research on the physician and patient dialogue around prescriptions should also include looking at these studies:
That is asking a lot of the money spent by the manufacturers on the physicians.
Detailing to physicians, nurse practitioners, and physicians’ assistants cost $12 billion, accounting for more than half of that promotional spending (see Figure 1). Drug companies spent another $3.4 billion sponsoring professional meetings and events and about $0.4 billion placing advertisements in professional journals. Pharmaceutical manufacturers spent the rest of their promotional budgets, $4.7 billion in 2008, on direct-to-consumer advertising.
December 20, 2012 0 Comments
One of the big issues in healthcare communications which is a rate limiting factor on health engagement is the language we use with patients. Here’s my attempt to talk about diabetes using different frameworks to drive home why this is important.
A clinical discussion:
You have diabetes mellitus. Because of that, you’re at increased risk for multiple co-morbidities including atheroscelerosis, hypertension, periodontal disease, retinopathy, neuropathy, and renal disease. Diabetes is considered a progressive disease. As our first line, I’m going to start you on monotherapy. Based on comparative effectiveness, this has the best clinical end points and lowest DUR issues. You will also need to maintain glycemic control and modify your physical activity level and caloric intake to minimize the long-term probability of getting ESRD and to lower your risk of myocardial infarction.
A mHealth discussion:
Based on our predictive algorithm and quantified self-tracking, I’m 90% confident that you have diabetes. To manage your diabetes, there are numerous widgets for assessing your risk along with online tools leveraging embodied conversational agents to support your efforts to self-monitor your condition. There are also apps which you can download which use gamification and location based services to address your intrinsic motivation to change. These tools will leverage the Trans Theoretical Model to understand your readiness for change and tailor messaging to you. Additionally, there are clinical staff available to help address your symptoms post-encounter.
A plain language discussion:
As you know, diet and exercise are important to maintain a healthy lifestyle. The test I had you take confirms that you have diabetes. Diabetes is a manageable disease, but it can lead to other health problems including gum disease, high blood pressure, and problems with your heart. We are going to start you on a prescription called metformin which will help to manage your diabetes, but you will still need to make some lifestyle changes. There are lots of technology tools on the Internet and your smart phone that can help you. I’d be happy to show you a few. They will help you track your calories, your exercise, and provide you with reminders about taking your medication. They can also help you learn about diabetes and answer some of your questions.
(And the above is at 7.8 grade level which is still too high for Medicaid and many programs.)
Here’s a summary from the CDC on Health Literacy…
What is Health Literacy?
The Patient Protection and Affordable Care Act of 2010, Title V, defines health literacy as the degree to which an individual has the capacity to obtain, communicate, process, and understand basic health information and services to make appropriate health decisions. This definition is almost identical to Healthy People. The only difference is the addition of “communicate” to the legislative definition.
Why Does Health Literacy Matter?
Every day, people confront situations that involve life-changing decisions about their health. These decisions are made in places such as grocery and drug stores, workplaces, playgrounds, doctors’ offices, clinics and hospitals, and around the kitchen table. Obtaining, communicating, processing, and understanding health information and services are essential steps in making appropriate health decisions; however, research indicates that today’s health information is presented in ways that are not usable by most adults. “Limited health literacy” occurs when people can’t find and use the health information and services they need.
- Nearly 9 out of 10 adults have difficulty using the everyday health information that is routinely available in our healthcare facilities, retail outlets, media and communities.1
- Without clear information and an understanding of the information’s importance, people are more likely to skip necessary medical tests, end up in the emergency room more often, and have a harder time managing chronic diseases like diabetes or high blood pressure.2
What Needs to Be Done to Improve Health Literacy?
We can do much better in designing and presenting health information and services that people can use effectively. We can build our own health literacy skills and help others—community members, health professionals, and anyone else who communicates about health—build their skills too. Every organization involved in health information and services needs its own health literacy plan to improve its organizational practices. The resources on this site will help you learn about health literacy issues, develop skills, create an action plan, and apply what you learn to create health information and services that truly make a positive difference in people’s lives.
References
1 Kutner, M., Greenberg, E., Jin , Y., & Paulsen, C. ( 2006 ). The health literacy of America’s adults: Results from the 2003 National Assessment of Adult Literacy (NCES 2006-483). Washington, DC: U.S. Department of Education, National Center for Education Statistics.
2 Rudd, R . E., Anderson, J . E., Oppenheimer, S., & Nath , C. (2007). Health literacy: An update of public health and medical literature. In J. P. Comi ngs, B. Garner, & C. Smith. (E ds.), Review of adult learning and literacy (vol . 7) (pp 175–204). Mahwa h, NJ: Lawrence Erlbaum Associates.
December 20, 2012 1 Comment
noun, plural trans·par·en·cies.
1. Also, trans·par·ence. the quality or state of being transparent.
2. something transparent, especially a picture, design, or the like on glass or some translucent substance, made visible by light shining through from behind.
3. Photography .
a. the proportion of the light that is passed through the emulsion on an area of a photographic image.
b. a photographic print on a clear base for viewing by transmitted light.
This is the dictionary.com definition of a term that gets thrown around in healthcare all the time. I’ve talked about transparency several times this year, and I expect a lot from companies like Change Healthcare in 2013.
That being said, I found an article in HealthLeaders in November 2012 very interesting. It referenced a study showing the answer to this question – “how will greater transparency on healthcare costs affect your organization’s cost of care”? I just assumed the answer would be that it would decrease costs. The data didn’t support that.
While 56% of health plans thought that transparency would decrease costs…
December 19, 2012 0 Comments
PAP programs (or Patient Assistance Programs) have been around for years. This is typically where a pharmaceutical manufacturer will set aside funds for their medications (theoretically) for those that can’t afford the medications. There are many other foundations and groups that will help patients to afford their treatment.
Interestingly, patients are now the biggest traffic draws on GoFundMe which is a crowdsourcing website for people to raise money. It leverages the power of social media to get the word out and draw people in. This replaces the local bake sales to raise money for individuals. A recent Time article (Crowdfunding a Cure by Alice Park) gave several examples of people raising money for surgery (e.g., $14,000) and cancer treatment (e.g., $144,000).
Of course, the risk here is fake diseases to steal money from caring people. The article says that GoFundMe requires a link to a legitimate Facebook profile and gated promotion beginning with an individual’s social network. But, in a world where we can buy Twitter followers, I’m not sure this really gives me much confidence. This seems like a great opportunity for an mHealth app to jump in and raise money that is directly paid to a provider and not collected by the patient. This would certainly limit some potential fraud and abuse.

Another site I found when researching this topic was GiveForward.

December 19, 2012 0 Comments
In a CNNMoney.com poll, 31% of those polled responded that “yes, it’s fine” to the question “are you happy with your health insurance”?
In the October 2012 edition, they shared a few other stats:
At the same time, healthcare costs continue to be out of control, and we need massive reform to a system that Americans aren’t excited about but yet have no fire forcing them to change.
December 18, 2012 0 Comments
Someone asked me yesterday if I could come up with 100 questions on one topic that I would want answered. I started by thinking about Rx adherence, but I evolved it to a broader topic (patient experience) to get to 100 questions. This is my list of 100 questions I would want to evaluate to understand the patient experience with a disease and what factors are relevant to segmentation and differentiation.
This exercise also led me to this equation as a strategic framework (not a mathematical algorithm…yet).
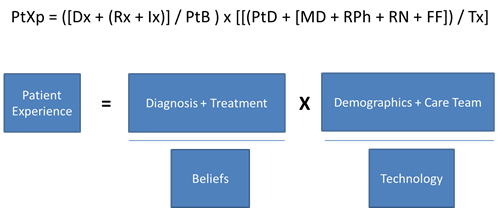
Patient Data (Demographics):
Patient Beliefs:
Diagnosis Attributes:
Treatment (Prescription) Attributes:
Care Team Attributes:
Technology Attributes:
December 18, 2012 0 Comments
For those of you that have read my blog for a while, I’ve talked about the possibility of augmented reality glasses several years ago before Google was talking about their offering (at least publicly). I still think one very cool use for this (in healthcare) is to create augmented reality shopping “paths” through grocery stores that are focused by disease state. For example, a diabetic could be guided to buy the best foods for them in the store.
You could also capture things that send them real-time to your case manager.
You could virtually pull a care-giver into your physician encounter.
Lots of exciting opportunities.
Here’s a cool video that some of you may have seen on Google Glasses which may be a consumer product before too long.
December 18, 2012 0 Comments
The tragedy at Sandy Hook Elementary School was a shock for everyone. In a connected world, it doesn’t take six degrees of separation to know someone who lost a child. I’m only one degree away from several people. And, for those of us with kids, it really makes you look at your school and their processes.
I wanted to take a moment to say that my thoughts and prayers go out to those families and the community and to capture a few thoughts.

General Thought #1: While we have a clear gun violence issue in this country (see infographic below), we’ve been slow to make any meaningful changes. Will this finally push us over the edge? I’m not sure. Certainly, those that like to own guns believe it might as you can see the sales of guns have spiked in the past few days. This seems like an opportunity for Obama to create a legacy for himself by changing this paradigm.
General Thought #2: The other big question or potential impact here is whether this will change the way schools or society in general deal with mental health issues. Even at the simplest level, I think about the stigma placed on people on anti-depressants. People who have depression don’t often openly discuss it, but the reality is that 16% of Americans are taking an anti-depressant (almost 1 in 5). If you assume there are many others that aren’t diagnosed or aren’t medicated, it becomes a significant population.
Interesting Video: The one thing I saw last night from a 9-year old was the video below which wasn’t made about Sandy Hook but was released and dedicated to them. It covers the broader topic of bullying and violence including school violence.
December 13, 2012 0 Comments
I’m not a diabetic, but I’ve been researching the topic to understand the space and what innovation is occurring around diabetes. This is a space where there are lots of applications, tools, devices, communities, and research. The ADA estimates the total US cost at $218B with very high prevalence. If you expand that on a global scale, the costs and impact is staggering.
So, what’s being done about it? And, what opportunities exist? I think you’ve certainly seen a lot of innovation events being sponsored by pharma and others.
You’ve seen a shift from drug to engagement for a few years as evidenced in this old post about Roche – http://www.diabetesmine.com/2009/10/a-visit-to-the-roche-new-concept-incubator.html
You’ve seen a proliferation of diabetes apps. (A prime opportunity for Happtique.)
From my traditional PBM/Pharmacy focus, you’ve seen several efforts there:
Obviously, Medco (pre-Express Scripts acquisition) thought enough of this space to buy Liberty Medical.
I pulled some screen shots and examples into a deck that I posted on SlideShare. I’d welcome people’s thoughts on what’s missing or what are the key pain points from a diabetes perspective (e.g., not integrated devices).
While I was doing my research, I found a few interesting things worth sharing.
Several interesting studies:
Some good slide decks:
Additionally a few videos:
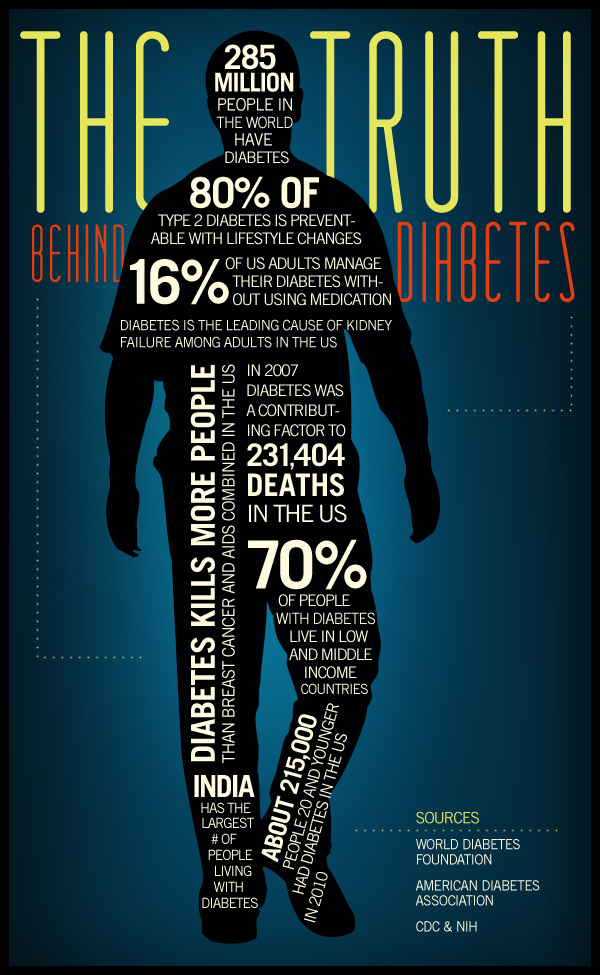
I also posted some diabetes infographics on my blog – https://georgevanantwerp.com/2012/12/13/more-diabetes-infographics/
And, while I started to pull together a list of diabetes twitter accounts below, you can follow @AskManny’s list with 360 people already tagged in it. https://twitter.com/askmanny/diabetes
My starting twitter List:
December 13, 2012 0 Comments
I’m sharing a few more here, but you can also go to Pinterest to see some shared there – http://pinterest.com/diabetesforum/diabetes-infographics/.

December 12, 2012 0 Comments
Our marketing team at inVentiv Medical Management created this infographic that I thought I would share.

December 11, 2012 0 Comments

Infographic by Healthcare Mobility Solutions Team at [x]cube LABS
December 10, 2012 1 Comment
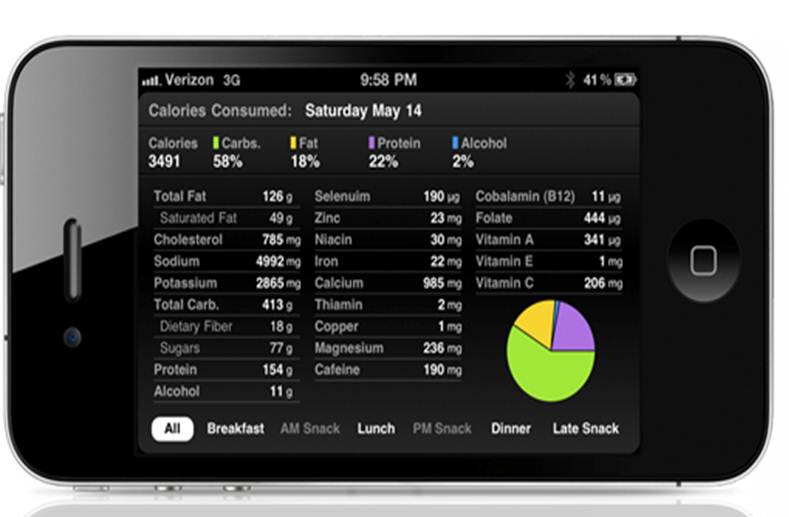
As someone who never tracked what I’ve eaten in my life (until recently with my FitBit), I’m just learning the value of this (more on another post). To that point, I was very interested in seeing several applications at the mHealth Summit last week in DC. While there are lots of different pros and cons, I sat down with Michael Segal from wHealthy Solutions (Wealth + Healthy) to talk about their FoodSmart app.
I found their application different and interesting based on the following:
FoodSmart’s new Custom Ranking feature gives people in special health populations a way to search the database by typing in a specific chronic condition. Users can search on the following categories to view custom rankings of food and beverages specific to these health concerns: Prediabetes, diabetes (type 1 and 2), weight management, hypertension and cardiovascular disease. Service functionality includes warnings about unhealthy ingredients; recommendations for healthier alternatives; user community taste rankings and reviews; personalized product lists; and the ability to create and share shopping lists with family members and other users.
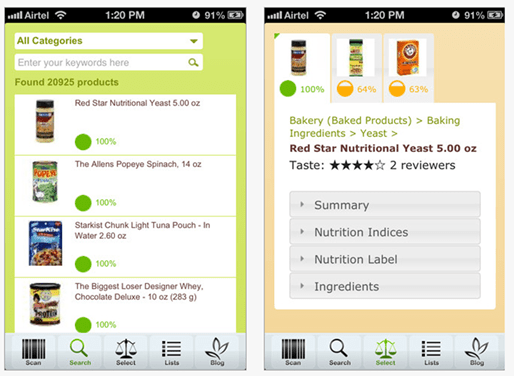
This is an interesting opportunity here since they’ve been growing primarily through viral growth. I talked a bit with Michael about trying to get incorporated into other applications and being used by nurses and others. I think that would drive adoption along with getting this to be something that dieticians would “prescribe” to their patients.
I will admit that it was fascinating to see how the recommendations change based on your disease. It plays well into what I think is important which is gradual change. For example, if I always eat cereal for breakfast, you might not change my habit, but you might get me to pick a better cereal.
December 10, 2012 0 Comments

Last week at the mHealth Summit in DC, I had a chance to sit down and visit with Christine Robins who is the CEO of BodyMedia. (see bio below) One of the most exciting things (mentioned at the end) is their new disposable solution coming out.
Christine Robins is currently the Chief Executive Officer of BodyMedia, Inc., a pioneering market leader in wearable body monitors. BodyMedia’s devices are unparalleled in the marketplace, and equip professionals and consumers with rich information to manage a range of health conditions impacted by lifestyle choices.
Prior to joining BodyMedia, Christine was the CEO of Philips Oral Healthcare where she led the global Sonicare® brand to significant sales and share growth. Christine also has extensive experience in a wide range of marketing and finance capacities gained during her 17 years at S.C. Johnson, where she ran notable brands such as Raid® insecticides, Glade® air fresheners, and Aveeno® skin care. With this background rooted in global multi-national companies and an entrepreneurial zeal essential to lead a high technology upstart, Chris is passionate about developing turnaround strategies, building teams, and driving innovation.
A noted speaker, Christine has delivered presentations at universities such as Harvard, Stanford and Duke, as well as keynotes at industry shows such as the Consumer Electronics Show, Health 2.0 and CTIA. She holds a degree in Marketing and Finance from the University of Wisconsin-Madison and an MBA from Marquette University.
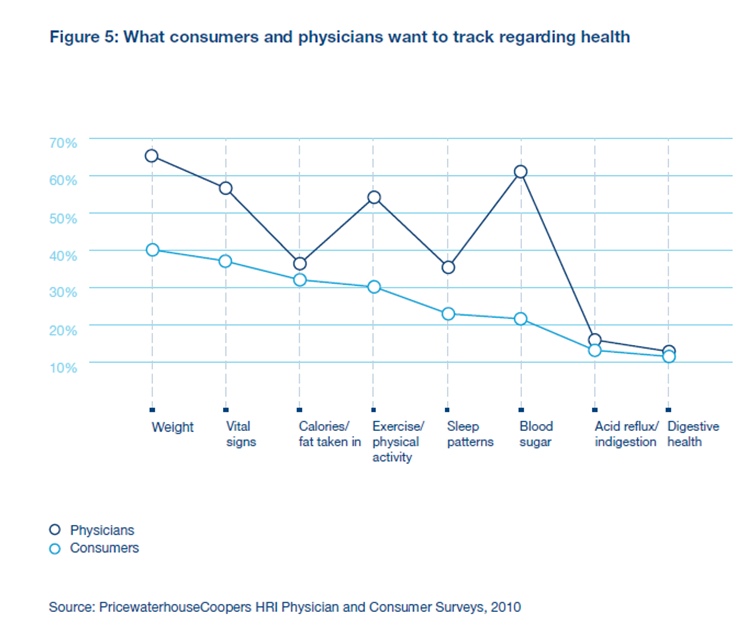
If you’re not familiar with BodyMedia, it’s definitely a company to know from a Quantified Self perspective. They have been around since 1999 providing solutions and have 150 global studies about the effectiveness of their devices in weight loss (see one chart below). The devices that they use continue to get smaller and smaller with time and are registered with the FDA as Class II medical devices.

Their devices track 5,000 data points per minute using 4 different sensors. Here are a few screen shots from the mobile apps that they have.

And, as you can see, they map well to the chart below which shows what data consumers and physicians want to track with weight, calories, physical activity, and sleep patterns.
For food tracking, they work with MyFitnessPal which provides them with data on products you eat. I think a good example can be seen in this screen shot from the Android app.
But, honestly, a lot of what I was really intrigued by was a new offering they’re rolling out called the “PATCH” which will be a 7-day, disposable body monitoring system that does everything the full blown system does. I don’t know the price point yet, but this is really exciting as a way to pull new people into the market and to use as a strategy for setting a baseline with a patient to understand their data. It could then lead to recommendations around disease management.
Another thing that Christine talked about was they’re approach to partnering with places like the Biggest Loser and other to allow for a customized content approach to your messaging from the system. She also showed me how the device will project where you will end up at the end of the day based on your past history.
They also have a module for a coach or weight loss professional to help manage and view data across all the people they’re working with.
(And, I just grabbed this image from their website since it points out the 3 key things to weight loss.)

December 7, 2012 1 Comment
I had a chance to sit down and do several interviews at the mHealth Summit earlier this week in DC. I’m slow to get my interviews posted, but they were all very interesting.
One of the best was with Dr. Bettina Experton (see bio below) of Humetrix. I will admit that reading about iBlueButton doesn’t do it justice. I was confused as to what they were trying to do and why it won an award. And, while explanatory after the fact, I found the graphic below intimidating as a consumer before talking with her.

[For those of you that don’t know what BlueButton is, you should go research it here.]
Dr. Experton explained to me how broad the BlueButton initiative now is. I only knew that CMS was using it, but apparently, there are now 200 plans also using it including Aetna, United Healthcare, and Humana. What Humetrix focused on for this offering was the mobile empowerment of BlueButton allowing the patient to have control of their information in the iOS platform (i.e., your Apple products – iPhone, iPad). They provide a tool for downloading and encrypting the data – prescription, medical claims, lab, and procedures.

Of course, if you’ve ever seen what this data looks like in the raw form, this wouldn’t seem very helpful. Most of us wouldn’t know what to do with this. But, as Dr. Experton showed me, they’ve rendered the data in a great GUI (graphic user interface) that really brings it to life in a readable and understandable format. For example, they translate the NDC code (used for prescriptions) into the drug name with the chemical name and the dosage. The GUI is very iPod like in terms of simplicity and ease of use.

The iBlueButton app even will pull in patient self-reported data from a PHR (personal health record) and show it in a different color and different section so the provider can understand the sources. Of course, this was another point of confusion for me before we talked which was how would a physician get this and what would they do with it. She showed me a demonstration of the patient opting to share their data and records with the provider in real-time. Of course, this assumes the provider’s office and/or the physician is actually using a device in the presence of the patient, but we know that is changing quickly these days. (See article on survey about MD use of iPad / iPhone.) So, with their tool, I can now store and share my data. The challenge still is integrating this data into the physician’s EMR (electronic medical record), but the iBlueButton app on the provider’s device can do this. It can also print it for those physicians who still want to see the printout in their paper file.
Another thing that you see in the second set of screen shots above is that you can start to report on whether you’re using the prescriptions still that it shows you on. Assuming patients engage, this would be a great tool for medication reconciliation and adherence discussions.
I’m not the Meaningful Use expert, but Dr. Experton pointed out to me that all of this is important since meaningful use requires viewing, downloading, and transmitting capabilities. They provide all of these.
I definitely plan to download iBlueButton and my data, and I hope to use this as a tool to reinforce why any claims provider should be offering you BlueButton access to your data. This is definitely a company to watch.
Bettina Experton, M.D., M.P.H.
President & CEO
Dr. Experton is the founder, President and CEO of Humetrix which she has led over the last 15 years on the HIT innovation path starting with the development of health risk appraisals, chronic care management software, and since the early 2000s with the development of novel mobile device-based solutions which have been deployed worldwide. A physician with over 20 years of healthcare informatics experience, Dr. Experton is the author of multiple information technology patents. At Humetrix, Dr. Experton also conducted groundbreaking health services research on the frail elderly which led to major federal legislation in the area of Medicare and managed care, and has been a national healthcare policy advisor in the US, China, and France. As a healthcare IT advisor to the French Ministry of Health, she made important contributions to the design of the newly launched French government sponsored single web-based individual health record with smart card access made available to French citizens and their physicians. Dr. Experton is an Adjunct Professor of Medicine at the University of California at San Diego, School of Medicine and a permanent member of the Faculty of the School of Medicine in Paris, after graduating Summa Cum Laude where she completed her training in Internal Medicine. In California, Dr. Experton received a Master’s degree in Public Health with a major in epidemiology from Loma Linda University School of Public Health, completed a Pediatrics internship at University of California Davis Medical Center and a Public Health residency with the State of California Department of Health Services.
December 4, 2012 3 Comments
I only had time to attend one day of the mHealth Summit in DC. Overall, it seemed like a well attended event with a good vendor area.
But, what I saw left me with concerns about the maturity of the space.
1. Every vendor has their own portal. There was no idea of convergence or sensitivity to the care manager or provider or patient having to access multiple sites to collect data. Of course, there were a few exceptions.
2. There’s still some heavy lifting for the consumer, but it’s getting better. For example, one food application lets you scan in your food but that calorie counter isn’t integrated into any activity monitor. Another application was trying to monitor social activity for part of their depression algorithm but they weren’t leveraging the data sitting on the phone itself – numbers of calls, movement, etc.
3. There are some really creative solutions being tried but the scale of the studies is small. I was excited to see what was being done with obesity, but the case studies were less than 150 participants.
4. There are a lot of non-healthcare people jumping in which is great from an innovation perspective, but healthcare is tricky and making sure to apply consumer literacy filters to the clinical guidance you get is important. For example, I asked one vendor why he had several chronic diseases covered but ignored high cholesterol. He pointed out that he had a heart disease component, but IMHO I don’t know many people with high cholesterol that would self select into heart disease.
On the other hand, there were some really positive things.
1. The user interface on a lot of these is very elegant.
2. The devices are getting smaller and smaller with a few disposables on the way.
3. The data captured and reporting is really interesting and insightful although I’m not sure how it will all be used by patients, physicians, or companies.
4. Technology is much more scalable than people centric strategies which is critical in the US and globally.
5. Several companies really get it and are focused on device neutral approaches for capturing and disseminating data.
Overall, it reminded me of some of my concerns about the Health 2.0 movement a few years ago in terms of business models and distribution models. But, keep the innovation coming. It’s fascinating and thought provoking. But, there will definitely be a shakeout in the years to come.
December 2, 2012 0 Comments

It’s always fun to predict what will happen in the next year. No one is ever right, but you can hope to be directionally correct. With that in mind, here’s a few of my thoughts for what will happen in 2013…
There are still a few longer term trends that I’m watching, but I don’t think that 2013 is the primary year for them.
December 2, 2012 0 Comments
If you read my interview with Michael Graves, it might have started your mind thinking about any of your visits to the hospital and all the problems you encounter. While many architects I’ve known have focused on the healthcare business over the years, I think it’s interesting to see the discussions of this topic move into more mainstream literature.
I was reading Fast Company’s article called Spaces That Heal which talks about redesigning hospitals (and it’s not their first article on this topic). It had several interesting points:
The article talks about HOK (where I did an architecture internship) and their project with the University Medical Center of Princeton to create a new patient room layout.
A related article goes on to provide more on the research on this topic…
Although architecture and design substantially contribute to patient and staff safety, efficiency, reduced infections, reduced patient falls, and improve patient and staff interactions, it has been found that music, aroma, and access to nature can alleviate stress for patients, families, and staff. Hospitals are increasingly providing access to green spaces or gardens, which have been proven to reduce stress (reducing blood pressure) and improve patient satisfaction for patients, families, and staff. Even viewing nature and trees has been shown to reduce hospital length of stay and result in fewer medications for patients.






