
I was reading the ScienceRoll blog tonight and saw this one entry on Health2.0 which posts the slides in a blog entry. Very cool.
Anyways, the blog is worth reading.
 September 28, 2007
September 28, 2007  0 Comments
0 Comments
I was reading the ScienceRoll blog tonight and saw this one entry on Health2.0 which posts the slides in a blog entry. Very cool.
Anyways, the blog is worth reading.
September 28, 2007 0 Comments
Assuming it is real…This is one of the worst stories I have seen about claims denial. Not only is it insulting, but it also shows how frustrating the process can be. (BCBSKC complaint)
“we have had Blue Cross and Blue Shield of Kansas City for less than three months, they have denied every claim we have submitted to them. EVERYONE!”
BTW – The blog here (The Consumerist) is pretty interesting. You might enjoy some of the entries:
September 28, 2007 0 Comments

I always enjoy getting e-mails from readers promoting new ideas or suggesting sites or events to look at. I received an e-mail the other day about iGuard which is a new company which is focused on delivering patient information about drugs as new information is identified.
It is interesting although I am not sure how much new information is discovered that is material, but when it is, I agree that I would want to know. Now, reading the website reveals that they have several concepts:
Now, it is important to blend this with a multi-modal delivery strategy which allows the patient to integrate this data into other systems they use and allows them to chose the channel for delivery – e-mail, SMS, fax, live call, automated call, letter, etc.
So, if interested, visit the website (www.iguard.org) and/or listen in to the webcast (see below):
iGuard
Live Webcast POWER TO THE PATIENTS!
The Most Up-to-Date Drug Safety Information
Sent Directly to You When You Need ItThursday, October 4, 2007 2:00 PM Eastern
Register Here!
September 28, 2007 1 Comment
Wellness is a big topic at employers these days. (And, it would be bigger if retention issues were fixed and companies knew how to retain their people.) The right programs can make people more motivated, healthier, and more productive and dedicated employees.
I found an example from eBay to be very innovative. They have launched a program called YourDinner.com which allows employees to spend a couple of hours per week (on the clock) with the company’s chefs assembling a week’s worth of dinners to take home. What a great idea! I get to save time and eat healthier and give my kids a good home cooked meal. (Not to mention it is probably a stress release.)
September 28, 2007 1 Comment
Here is a good example I found yesterday in Fast Company that reinforces one of my posting from a few weeks ago on loss avoidance.
In an article that talks about plastic bags and how bad they are for the environment. Would you believe we use 380B of those plastic bags you get at the grocery store (each year)? And, in landfills they last 1,000 years. I could go on, but that’s not the point of this blog.
Anyways, at Whole Foods, they give the customer a $0.05-$0.10 discount for each bag they reuse (i.e., reward). They get 20% of people bringing in their own bags. Ikea charges customers $0.05 for each bag they take (i.e., loss avoidance). Ikea utilization of plastic bags has dropped by 50%. People hate to lose more than they like to save.
September 26, 2007 2 Comments
If you have never read Penelope Trunk’s blog, you are missing out. She is one of my favorite bloggers and has good, controversial opinions about worklife.
I think we all wonder about the correlation between health and professional (and personal) success. She has a good blog entry today about being overweight.
“Heavier people do worse at work than everyone else, employers discriminate against overweight people, and it’s even legal to do.”
As health drives cost and impacts performance (e.g., missed hours), people consciously or subconsciously pay attention to it. We could debate endlessly the ethical issues here, but let’s stick with reality. It happens. So, how do you address it.
Some people don’t like smokers. Some people worry about people that are chronically absence. Others realize that caring for a sick kid impacts their entire team.
September 26, 2007 0 Comments
In yesterday’s USA Today, there was an article by Rita Rubin called “Routine exams may need checkup“. There were some interesting points:
I guess the questions here are:
September 26, 2007 0 Comments
JAMA just published a study on treating depression and its impact. Here is the summary from the Associated Press which hits the highlights. With 6% of the population having depression and estimates that this costs our economy $30B a year, this is a big deal.
“Investing in depressed employees _ quickly getting them treatment and even offering telephone psychotherapy _ can cut absenteeism while improving workers’ health, a study suggests.”
What did they study:
This seems like an obvious one. There are lots of therapy specific instances where we can take a more aggressive outreach to impact health and bottom line. The best way to get a program launched is have a value prop that addresses both issues.
September 24, 2007 0 Comments
The more I use the healthcare system the more I realize the issues with the system. While I was preparing to take my new job, I went temporarily on COBRA. I ended up with a few paper claims while I waited for my new insurance cards and due to an eligibility file issue which the MCO or the TPA made.
Now, I am trying to get reimbursed for the 5 prescriptions for my family. After filling out the forms and getting the pharmacist to sign them, I faxed them to my payor. A month later, I have heard nothing so I called them. They inform me that they have been processed, and I will get a check less my copay. (Sounds great.)
Then, they walk me through the claims. In one example, I paid $95 for a generic drug. Well, their negotiated rate with the pharmacy for that drug is $22. Taking out my $10 copay, they are sending me a check for $12. WAIT! What about the other $73 that I spent (times 5). I got a nice lecture on negotiated rate versus retail which I explained to the woman that I knew.
(Here is a WSJ article on generic pricing. This is where the margins exist. Cash customers often pay the average wholesale price plus while the negotiated rates for the payors are usually 60% or more below the average wholesale price. Here is a blog discussion in the Freakonomics area about prices ranging from $12 to $117 for the same generic prescription.)
All I care about is getting my cash back. They can refund my premium, claw it back from the pharmacy, or write me a check. They didn’t get me my cards or set me up right (or the Third Party Administrator (TPA) didn’t). I don’t care.
After a second call, they inform me that I can appeal it and will hear in 30-days at which time I can appeal it again. It makes me ask what the problem is and how this works for people with limited cash flow. You have to pay and wait 3 months only to likely get turned down. This seems like a major flaw in the process. Why offer paper claims if you don’t get your money back?
September 23, 2007 0 Comments
I have been a big fan of Myers Briggs for years. Every since I took the test and realized that it described me to a tee. I even took an elective in graduate school to drill down on the testing and look at ways to use it in team development and other activities.
The purpose of the Myers-Briggs Type Indicator® (MBTI) personality inventory is to make the theory of psychological types described by C. G. Jung understandable and useful in people’s lives. The essence of the theory is that much seemingly random variation in the behavior is actually quite orderly and consistent, being due to basic differences in the ways individuals prefer to use their perception and judgment. (source)
If you haven’t taken the test, here is a site where you can answer a page of questions. I took it and it matched my end result from numerous testings. So why bring it up here? And, why is this entry 1 of X?
First, I am a big believer in trying to categorize individuals to make some assumptions about how to deliver healthcare information to them. This is one theoretical attempt to do this. Second, I am certainly not going to solve this tonight so I will layout a few thoughts and likely pick the topic up again.
The first category is Introvert (I) or Extravert (E). For me a healthcare introvert is someone who doesn’t talk about their family history or their individual ailments. If they feel sick, they will research it before making an appointment. Additionally, they may read online discussion groups but won’t participate. The extravert will ask everyone’s opinion about their condition. They want to tell you their cholesterol. If they feel bad, they go right to the ER or Urgent Care. And, if they have a chronic condition, they are active in online or physical groups.
The second variable is Sensing (S) or Intuitive (N). For me, the sensing healthcare person has a deep memory of their condition. They can tell you (and may even record) all the facts about their experience with a provider, drug, or disease. The intuitive healthcare person remembers the general patterns (e.g., every time I eat after taking my pill) and speculates on what this might mean. They aren’t focused on the specifics but more on the possibilities.
The third variable is Thinking (T) versus Feeling (F). The thinking healthcare person is consumed by the facts. They want to read the medical research and debate with their providers the treatment plan based on an article in the New England Journal of Medicine. The feeling person is much more driven by experience. If the placebo is helping them, they are willing to stick with it. Or, if their neighbor says that generics are not good, then they won’t buy generics.
The final category is Judging (J) or Perceiving (P). The judging patient is planning their care path or wellness. They participate in disease management. They go to preventive clinics. They get the flu shot even if they never get the flu. The perceiving person reacts to the events. They don’t have regular check-ups unless they are in pain. They don’t participate in any programs unless they are sick.
These are some initial thoughts, but we all know that figuring out a healthcare segmentation model that would predict behavior is significant. I don’t have the answer, but I think there is something here.
If you know your type and want to learn more, here is a good site I found. (http://typelogic.com/)
September 23, 2007 0 Comments
In a special Business Week Report, Joseph Paduda (who writes the ManagedCareMatters blog) provides a critical summary of CDHPs (see CDHPs: No Rx for Health Care). I think he makes several good points (although some of the commentors seem to disagree).
“The concept behind CDHPs is simple: People will be more careful about choosing which health-care services they buy if a big chunk of the dollars comes out of their own wallet.” [As I have said before, I thought the original intent was to drive transparency and improved quality, but it is clearly about cost shifting (oh sorry I mean savings) today.]
“A RAND Corp. study concludes that when individuals are required to pay more for prescription drugs, they don’t take them as they should. As far as drug co-pays go, increasing consumers’ costs actually drives up total medical expenses. It’s not a great leap to think individuals with high deductibles will likely wait before scheduling an appointment with their physician to see if a problem just goes away on its own. That often leads to higher costs as the patient’s medical condition worsens and grows more difficult to treat.”
September 23, 2007 1 Comment

No, I am not taking money to do advertising. After seeing this Comcast advertisement on TV about 3 times, I finally got what they were trying to say. Some made up word of “televisiphonernetting”. In the commercial, there is a guy talking on the phone while web surving and watching TV. The grandfather is trying to talk to him with no luck.
This is a good reality to think about when trying to communicate with consumers. We are consumed by our busy lives and always multi-tasking. Finding the right medium, timing, and message to get them to give you 10 seconds of time is difficult.
In healthcare, we have lots of opportunities to touch the patient. The key is doing it around an event. They are engaged for a brief period of time around a visit to the doctor or getting a prescription or going to the lab. If you can trigger messages that are targeted to their situation and timely, they will engage. General educational messages that aren’t personalized or timely often fall on deaf ears.
September 21, 2007 2 Comments
This week was the Health 2.0 Conference in San Francisco. I was not there, but I am sure it generated a lot of good discussion. Numerous bloggers were there and put there comments up. Here are a few sites for content. It is certainly worth the read if only to keep up on new technology and new buzz words. But, getting together a group of technologists focused on changing healthcare can only lead to some new ideas.
September 21, 2007 1 Comment
After trying a few entrepreneurial things, I am excited to have accepted a job working with a consulting client of mine – Silverlink Communications. [I am also a former client of theirs from my time at Express Scripts.] The role is a good mix of entreprenerial and stability since they are a high growth, VC backed company. And, one of the most impressive things is their track record of delivery and impressive clients including lots of the big MCOs and PBMs (examples).
As I was getting ready to do an e-mail blast out to a 1,000+ people in my Outlook database, I figured that linking them to the blog and answering their predicted questions here might be a good solution. I could go with the micro-segmentation of my audience (i.e., my healthcare friends want to know something different than my consulting friends) that I started to do, but it’s turning out to be more time consuming than I would like.
So here goes. Here is more information about what I am doing and why. If you are in the healthcare space, I would encourage you to look at Silverlink and give me a call. We can leverage our technology and services to help you cut costs, grow revenue, and inprove patient satisfaction and outcomes.
Q&A:
[Official PR Text] Silverlink is the leader in automated voice solutions for healthcare enterprises. Silverlink’s services enable customers to design, deploy and manage HIPAA compliant automated call programs to educate, collect information from and drive behavior of thousands of patients and members at a time. Serving six of the top ten health plans and with a customer base that collectively represents over 150 million covered lives, Silverlink drastically reduces the cost of communicating with customers while improving financial results and customer care.
We saw great results at Express Scripts. In one controlled study we ran through research, we saw our success rates improve by 30% by blending letters and calls. Additionally, access to data and flexibility were critical. We launched one new call program in under a day (either for Katrina or for a new drug warning).
Everybody is talking about consumerism and Health 2.0. Silverlink plays right into that strategy. Delivering timely information to patients. Blend their core technology with multi-modal, data mining, and experience based branding, and you have a unique opportunity to change the paradigm.
I am sure I could go on. But, while you are here, I would encourage you to look at the Silverlink website (PBM, MCO, Medicare, Medicaid, DM, Specialty/DME) and also at rest of my blog. If interested, register to get updates to the blog via e-mail by clicking here.
September 21, 2007 0 Comments
In case anyone is interested, I have had a few people ask me if I knew anyone interested in the following:
September 20, 2007 0 Comments
I must admit that I haven’t read the book yet, but it has been recommended to me by several people. (Married to the Brand) 
Instead [of volume or profit], companies should focus on an objective that merits the diligent, even obsessive attention of the company’s managers: customer engagement, and healthy brand marriages. Every manager should be laser-focused on building and protecting the company’s most precious assets — its powerful and passionate customer relationships. These brand relationship assets determine the continued health and future success of the company. (see more on the book content)
The reason I mention it is that in talking with an experiential branding expert I found their example of Starbucks very comparative to healthcare. It has died down a little in the past few years, but I have often heard people talk about how hard it is to differentiate a healthcare offering. I think Starbucks is the perfect example of a different way of thinking about this.
Coffee is coffee (with some slight modifications in taste). People go to Starbucks and one of their sustainable differentiations is the experience. It is difficult to replicate the experience that people have. That should be the focus in healthcare. How they experience the office lobby, the staff, check-in, admissions, enrollment, the call center, member materials, outbound communications, etc.? This is what will make you different.
It is never easy to quantify loyalty and correlate that with experience. But, let me use a simple example. I bet that price being relatively equal no company will switch health plans, PBMs, etc. if the CEO and/or their spouse has had a great experience with the company. There are too few great experiences. This is your chance to step-up.
September 19, 2007 0 Comments
I was reading through the WSJ blog on healthcare and found an interesting item around medical records being the new credit score. It’s a good point. With people’s sensitivity around getting insurance coverage, you certainly don’t want to have a mistake in your healthcare information (at least not one that makes you appear more sick).
With all the manual data entry in healthcare, I would not be surprised that this happens.
Here is the blog entry.
September 19, 2007 2 Comments
There are several models for dispensing drugs. I talked about kiosks the other day. Obviously, there is a physician dispensing also. In this case, the physician stocks and fills drugs for patients and collects cash payments. They can make good money, but it can represent a (perceived) conflict of interest and present some challenges (e.g., space, cash management, drug-drug interactions). Several companies that help this model are Allscripts, Dispensing Solutions, and Purkinje.
Another model which is very interesting, but it hasn’t taken off is generic sampling using physician kiosks like MedVantx. It is a cool technology. And, since generic manufacturers don’t provide samples, it is a good way of starting therapy on a generic drug. (The reason for pharma using samples is to get the patient started on their drug.)

Some scary data and a good discussion on this topic can be found on the Medinnovationblog.
Each pharmacy call back costs physicians’ practices $5-$7. With the average physician writing 30 prescriptions a day and handling another 30 requests for refills, the costs escalate rapidly. The estimated 20 pharmacy related phone calls per day costs $20,000-$28,000 annually. In general, physicians are oblivious to this cost center. By moving dispensing into the physician’s office, this overhead can be cost shifted to better serve patients as well as create additional income.
September 19, 2007 0 Comments
I was looking at the Healthwise website and The Center for Information Therapy and came across a blog by the team there with some good discussion topics. It is definitely worth your read. Here were a few things that caught my eye:
September 19, 2007 0 Comments
Excuse me while I rant for a moment. I spent the night at a below average hotel last night. The air quality was horrible. At first they put me in a smoking room. I didn’t even know they still existed in hotels. I thought I would choke when I entered the hallway. (If I hadn’t prepaid on Travelocity, I would have left.)
Even though they moved me, I think it is an issue throughout the hotel since I woke up with a sore throat and headache. To top it off, the hotel doesn’t even have a workout facility.
In today’s wellness environment, I figured things like this didn’t exist (at least not at normal chain hotels).
September 19, 2007 0 Comments
Wells Fargo and Gallup put out the results of a poll of small business owners last week that underscores just how challenging it is for them to provide healthcare coverage for their employees even though they clearly know this is an important benefit in attracting the right type of talent.
A few of the key facts from the study are:
Here is a good quote from a Wells Fargo executive:
“The majority of small business owners recognize the benefits of offering affordable healthcare coverage to their employees, but many feel they cannot afford to do so,” said Rebecca Macieira-Kaufmann, executive vice president and head of Wells Fargo’s small business segment. “A third of small business owners are cutting back on non-capital investments so they can provide healthcare for their employees. For several years health insurance has been a major concern for small business owners, and its impact is significant.”
Since small business is where much of our job growth has been over the past decade, this should raise flags for us. I think it is critical that we find a solution that creates easily accessible healthcare for everyone, but I think it is ridiculous that working families can’t afford care or aren’t provided care.
September 18, 2007 0 Comments
As anyone who has done anything outside normal knows, getting and managing your medical claims can be very confusing. When should you pay? When should you resubmit? When is it simply an error?
I was encouraged to learn about a new company MedBillManager which has recently secured some funding. They have a blog where you can read some thoughts and you can read about them in a WSJ article. The WSJ points out other companies such as WebMD, RevolutionHealth, and Intuit that provide tools to help get you organized and/or provide information.
Here is a screenshot. The team there offered my readers a free one year subscription ($24.95 savings). Go to https://prod.medbillmanager.com/account/signup and click on the “Got a free plan code? Claim it” link… enter in gvareader1. I think they would welcome the feedback.
Much like the OutofPocket.com that I blogged about the other day, this is heavily dependent upon adoption to drive value. Being able to compare costs by treatment, geography, insurer, and physician is valuable long-term in a consumer driven world, but it needs participation to have enough detail at at specific segment.
The other key for success will be integration of data directly from the payors. I don’t mind entering a few EOBs and bills to see some data, but eventually, I want them to be pre-populated and then use the application for reporting and analysis. Blend this with a technology such as that from ActiveHealth and a PHR and you have an integrated data selection that tracks costs, compares data, and pushes suggestions to you about wellness and health management.
This is probably what RevolutionHealth is doing. I am sure we will see some more rollups over the next few years to pull all these solutions together.
September 17, 2007 0 Comments
I enjoyed Sicko. The movie made you think. All information comes with perspective.
20/20 had a good piece the other night which showed John Stossel talking to Michael Moore and bringing up lots of interesting facts about Canada and Cuba and asking tough questions. It was a good opposite view.
Rather than rehash, I will point you to Kevin MD’s Blog which has links and provides some other blog summaries.
September 17, 2007 0 Comments
In an interesting, if not over my head conversation, Robert Goldberg (VP of the Center for Medicine in the Public Interest) talks about comparative effectiveness which effectively looks at the costs of treatments versus the outcomes. From a business perspective, this makes all the sense in the world.
On the flipside, I certainly understand his key arguement which points out that generalizations don’t work. A drug that doesn’t work generally might work for a certain minority segment. I pulled a few quotes below, but you can read the whole Washington Times editorial here. This is why genomics is so important. Once we understand how drugs and treatments vary by genes and understand what genes each person has, we will be much more effective at treatment and outcomes. (I am not so sure about cost, but we will table that for now.)
September 17, 2007 1 Comment
Everyone is moving to self-service. Quicker. Cheaper. Privacy. Automated. Etc.
There are lots of benefits. Think about all the information which is needed in healthcare along with all the linked processes. If this can be simplified and some of the burden pushed to patients that is great.
Now, this will vary by age and demographic. Typically older people will be more hesitant to use automated technology. Just look at your self-service grocery lines. Additionally, you have to watch interpretation of questions. I will never forget the doctor asking my grandfather if he smoked and him saying yes. I asked for a point of clarification and found out he had smoked 35 years ago.
I couldn’t find all the examples, but I have talked with vendors using kiosks for checking in to an office or hospital, providing translation services, helping match basic needs with over-the-counter medications, simplifying basic services (e.g., picking up a refill prescription), or for pushing information to the patient.
Kiosks blend challenges with physical design (height, location, screen size) with application challenges (number of screens, simplicity, data entry) with business model challenges (costs, advertising (Y/N), patient utilization). But, done right, I clearly see this as key to the future of healthcare. It will help address staffing shortages, address data quality, and help patients take on more responsibility.
Imagine walking up to a kiosk and using biometrics (i.e., retinal scanner, fingerprints) to log-in. Once you log-in, your history (Rx, lab, medical) is all available via your personal health record. You register for your appointment and get pushed health and wellness information that you can print real-time. You can then chose to print information for discussion with your physician based on monitoring of your cholesterol, weight, and blood pressure for your home system. Finally, because you log-in, the system automatically queues up other events for the staff to initiate pending your visit with the doctor.
Here are a few examples of kiosks in healthcare:
And, if you’re really interested in kiosks, you could read Bill Gerba’s blog on kiosks.
September 16, 2007 0 Comments
Next year’s election for president should have healthcare as a key issue. It has certainly become a front page issue. Do you focus on universal coverage? Do you focus on the uninsured? Do you focus on errors? Do you focus on quality? Do you focus on consumerism?
It will be very interesting. If interested, I am not going to summarize everyone’s opinions, but here are a few links that will provide you with more information:
September 16, 2007 2 Comments
The Institute of Medicine published a report a few years ago called “To Err is Human” which should scare all of us. There has been some debate on the facts, but here are a couple of critical findings:
So, the question in my mind is what is being done to educate the consumer about how to avoid errors. Systemically, I know there are several things being pursued. But, it is easy to be the victim of an error. I had two prescription errors in one year from my local Walgreens. First, they gave me ear drops for my eyes. Second, they gave me a antibiotic for my son which wasn’t filled with enough water.
When I was looking around for advice, I found these 20 tips from the Agency for Healthcare Research and Design. They highlight several things which in many cases boil down to asking questions:
I also saw several other interesting things at the Agency’s website such as a Pocket Guide to Good Health for Adults.
You can also find more information about prescription safety from the Institute for Safe Medication Practices.
September 14, 2007 0 Comments
Anyone working in healthcare IT knows it is difficult to drive change – legacy systems, lots of constituents, no standards or years of trying to get one, regulatory issues, etc.
I liked Scott Shreeve’s letter to Marissa Mayer who is apparently taking over Google Health with Adam leaving. As one might expect, Google‘s presence in healthcare leads to lots of rumors. I saw one earlier today talking about them buying WebMD (rumor).
Scott hits on several things:
September 14, 2007 1 Comment
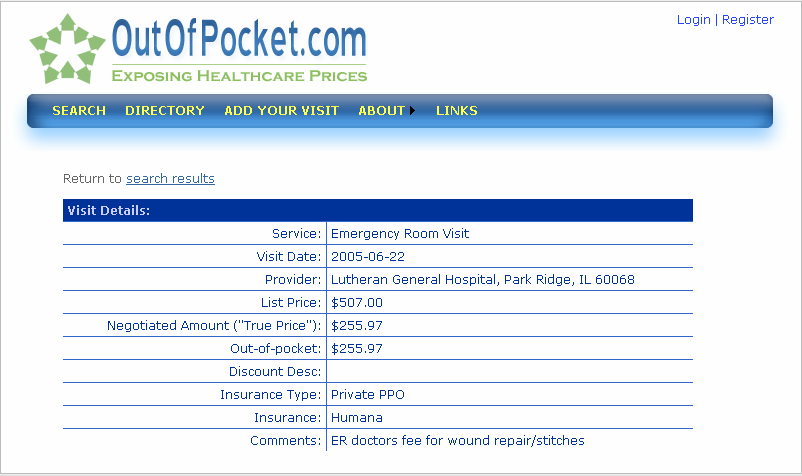
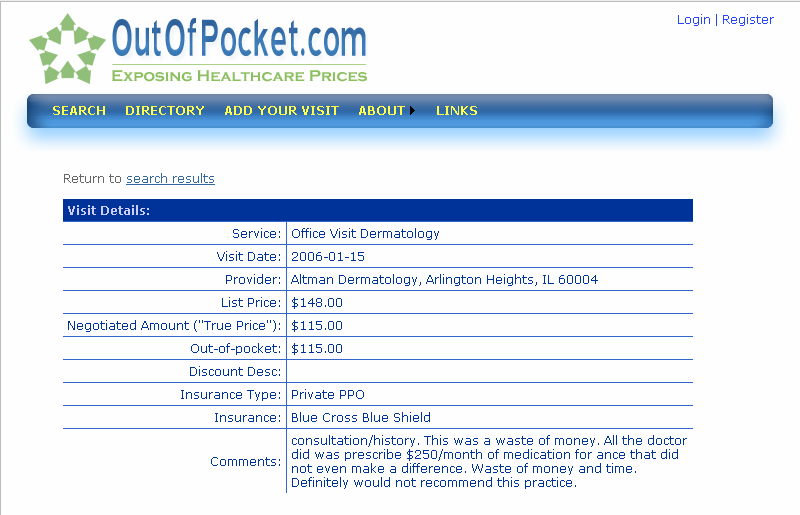
Obviously, a big part of true consumerism will be patients sharing information about their healthcare experiences (e.g., this doctor is great, you wait too long here, this drug gave me hives) and their costs (aka transparency). There are several locations moving towards this especially around disease specific discussion groups.
One new site that contacted me is OutOfPocket.com. It is still very early stage, but it has the right concept. You can go online and look up the comparative costs of a treatment or office visit in your area. Below are two examples. I like the second one where the patient cuts to the chase in the comments area. The company also has started a blog recently which I look forward to being cutting edge and aggressively laying out cost data.
September 14, 2007 0 Comments
I had an interesting discussion earlier this week. The question was whether people view their healthcare companies as a financial company (i.e., cost is the dominant factor and/or the cost to value tradeoff) or as a service company (i.e., my experience at the doctor’s office, hospital, pharmacy, call center).
I am sure it is not universal, but it would be an important attribute to understand in driving communications with patients. The easiest example I always use is the paper claims process. Imagine getting rejected at the pharmacy and having to pay $200 for your prescription. For some, $200 is a huge cash flow issue while for others it is simply a nuisance. Where that person is coming from will vary their perception of that same experience dramatically.
For the person with the $200 cash flow issue, a reject forces them to either tradeoff medications versus food or heat. Therefore, you are denying them care and possibly causing them harm. For the other person, they pay the cash and are simply ticked off. For them, it then becomes a customer service issue of how easy it is to submit a claim and how quickly they get reimbursed.



