
I am checking out on vacation for a week. I don’t expect to be doing any blogging. I will try to catch up when I return.
Archive | July, 2008
Gas Prices Helping PBMs
 July 24, 2008
July 24, 2008  1 Comment
1 Comment
Unfortunately, the WSJ Health Blog beat me to it, but I think it’s an interesting perspective that apparently David Snow (CEO of Medco) talked about. High gas prices cause people to reconsider things…like driving to the pharmacy or paying for brand drugs. That would mean that mail order penetration should go up and people should use more generics.
It seems logical, but I am trying to reconcile it with two other economic realities…people not filling their prescriptions or skipping doses to save money and the fact that mail order requires upfront payment for the longer supply. I have always struggled with why someone doesn’t offer a credit card for their mail order pharmacy so that you can save money and spread the payment over three months. In tough economic times, that cash flow can be an issue.
And, for the first time in over a decade, it appears that the growth in prescriptions actually fell as reported on the 16th in the WSJ.
The burden on consumers has increased sharply. The average copay for a preferred drug on an insurance company’s tiered system rose 67% to $25 in 2007 from $15 in 2000, according to the Kaiser Family Foundation. Out-of-pocket costs to cover family insurance premiums were $3,281 per employee last year, up nearly 84% from 2001.
Consumers appear to be skimping on medicines as a result. An April poll from the Kaiser foundation showed 23% of patients who responded didn’t fill a prescription in the last year because of cost, up from 20% in 2005; 19% split pills or skipped doses, up from 16% in 2005. A report last month from the nonpartisan Center for Studying Health System Change in Washington, D.C., said 20% of respondents in a 2007 survey of 18,000 people had put off or gone without medical treatment in the previous year, compared to 14% in 2003.
Data from IMS Health show growth in prescription volume for the first five months of this year slowed to 1.5%, the lowest rate at least since 1996. From 2003 to 2007, annual volume growth averaged 3%. In December 2007, total prescriptions dipped by 2.1%. The decline was 0.2% in April and 0.1% in May.
Traveling With Autistic Kids
July 24, 2008 0 Comments
After the incident a few weeks ago when a mother was kicked off a plane since her autistic child was uncontrollably upset, I was glad to see the article in USA Today about this challenge. It has some helpful information such as the fact that 1 in 150 kids have autism and 1 in 94 boys have autism.
The recommend the following:
- The Autism Society of America sells wallet cards, left, that describe common characteristics of autism and tips for interacting with autistic children that parents can give to airline personnel.
- Visit the Department of Transportation website to read the Air Carrier Access Act, which outlines the rights of disabled passengers.
- Prepare for the trip by showing your child pictures of the airplane, the terminal and the destination.
- Alert the airline that you will be traveling with an autistic child. Many airlines will allow you to board first.
- Choose a vacation destination that will accommodate your needs. Many parents recommend Disney World, which is known for its disabilities services.
Since some of their reactions (to what most of us adults hate also) can look like misbehavior by children, I can only imagine the looks that the parents get. As the article suggests, look and think about how you can help…don’t judge.
Cell Phones and Cancer…Cautious?
July 24, 2008 1 Comment
In another confusing story to us the public, everyone has picked up the story about the head of a prominent cancer research agency telling the employees to limit their mobile phone usage.
“Really at the heart of my concern is that we shouldn’t wait for a definitive study to come out, but err on the side of being safe rather than sorry later,” Herberman said. [Dr. Ronald B. Herberman, director of the University of Pittsburgh Cancer Institute]
The suggestion is to limit use for children to emergencies, use hands-free devices, and use speaker phones. The article cites several studies and the FDA saying that there are no issues.
Of course, this makes me think of autism and vaccines. Is it an issue or not? It also begs the question and the social responsibility of the health care system on whether to encourage us to be cautious or wait the decades for definitive research.
Love What You Do
July 22, 2008 1 Comment
We had an annual company event today, and I must admit that all day long I kept thinking about when can I get back to my hotel to work on several ideas that I have and get a couple of deliverables out the door. Not that I wasn’t having fun since it was one of the best company events I have been to. But, I love what I do. And, since I have had the chance to work several places and even more as a consultant, I think being happy at work and enjoying your corporate culture is very important.
I love that fact that the company takes the time to celebrate and discuss the future. And, it is great to be at a company that is still of a size that everyone can interact with each other, but big enough that you can make investments in the future. Anyways, working on a few things for some of you clients and enjoying every minute of it.
But making it relevant for the rest of you…it made me think of the correlation between job satisfaction and health. We all know the problems with stress and the impacts on health, but I found what looks like a good meta-study that shows the correlations. Here is the abstract fromOccupational and Environmental Medicine 2005;62:105-112.
The relationship between job satisfaction and health: a meta-analysis
E B Faragher, M Cass, C L Cooper
Background: A vast number of published studies have suggested a link between job satisfaction levels and health. The sizes of the relationships reported vary widely. Narrative overviews of this relationship have been published, but no systematic meta-analysis review has been conducted.
Methods: A systematic review and meta-analysis of 485 studies with a combined sample size of 267 995 individuals was conducted, evaluating the research evidence linking self-report measures of job satisfaction to measures of physical and mental wellbeing.
Results: The overall correlation combined across all health measures was r = 0.312 (0.370 after Schmidt-Hunter adjustment). Job satisfaction was most strongly associated with mental/psychological problems; strongest relationships were found for burnout (corrected r = 0.478), self-esteem(r = 0.429), depression (r = 0.428), and anxiety(r = 0.420). The correlation with subjective physical illness was more modest (r = 0.287).
Conclusions: Correlations in excess of 0.3 are rare in this context. The relationships found suggest that job satisfaction level is an important factor influencing the health of workers. Organisations should include the development of stress management policies to identify and eradicate work practices that cause most job dissatisfaction as part of any exercise aimed at improving employee health. Occupational health clinicians should consider counselling employees diagnosed as having psychological problems to critically evaluate their work—and help them to explore ways of gaining greater satisfaction from this important aspect of their life.
Keep The Change
July 22, 2008 0 Comments
I was listening to an advertisement for Bank of America’s Keep the Change program this afternoon and found it to be very interesting. Essentially, every purchase you make with your debit card gets rounded up and the difference put into savings. For example, if you spend $3.43, they bill you $4.00 and put $0.57 in your savings account. Forced savings (post opt-in of course). And, they even having a matching program.
So, this accomplishes several things:
- Creates an easy way for the consumer to save
- Increases the money saved at Bank of America
It’s certainly in the bank’s best interest and good for the consumer. It gets me back to my question from the other day. If you are driving a positive result but you have to force the consumer there, is that okay?
What’s the healthcare model of this?
- If you implement (or do) all your preventative care recommendations, your prescriptions are free (or some type of incentive system like this)? Which is good for the payor, insurer, and patient.
- How about a bundled copayment for certain events which included the office visit, hospital charges, and the prescriptions? (Oh…sorry we couldn’t do that since we don’t know the prices in advance.)
New Drug Trend Blog
July 18, 2008 0 Comments
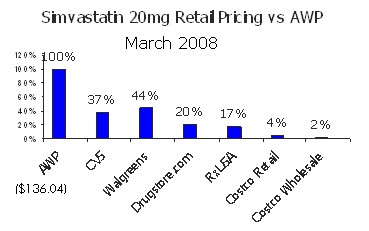
In a new blog called DrugTrendsToday by DestinationRx, you can find some good initial posts and some good data such as the following on generic Zocor (aka simvastatin). What this shows you (that I have blogged about before) is the massive difference between AWP and actual cost for a generic. In this case, the AWP is $136, but Costco pays 2% (or $2.72) for the drug. This huge difference is only true on generics, but unfortunately, the industry has come to depend on generic pricing as the profit engine to subsidize the brand pricing which is some cases is a loss leader.

460,000,000 Vacation Days
July 17, 2008 0 Comments

Just a nugget I came across. (If you can’t tell, I am trying to clean up my inbox today.)
According to Expedia.com, US employees will leave 460M vacation days on the table in 2008. Pretty sad considering the value of those days and their ability to help us manage our lifes and stay balanced.
RWJF on PHRs
July 17, 2008 0 Comments
The Robert Woods Johnson Foundation has put out a series of podcasts on Personal Health Records. I love to see how people are using new media more and more to deliver information.
PBM Competitive Intelligence
July 17, 2008 0 Comments
TMA, a group that was doing a PBM study, called me with questions a few months ago. They sent me some of the results of the work last week. A few interesting observations from them looking at CVS Caremark, Medco, Express Scripts, Wellpoint NextRx, Prescription Solutions, Aetna Pharmacy, and CIgna:
- Aetna was cited as having the best online capabilities.
- Express Scripts was cited as having the best generic drug conversion.
- Medco was cited as having the best disease management.
- Medco was cited as having the best sales channels.
- CVS Caremark was cited as having the best practices for implementation.
“As competition among PBMs is forecasted to remain high, customer service will continue to become more and more important as members/patients have greater expectations.”
Call Center Agent vs. Automated Calls
July 17, 2008 0 Comments
The other day I called some service provider to ask some questions about their product. It was painfully obvious that the person at the call center was reading from a script. This made me realize that there are reasons (beyond simply cost) for using automated, speech-recognition technology for calling people versus humans.
 It would have been more conversational for me to have talked with an automated phone call where I could answer questions with certain hotwords that dynamically moved me through the path of the call. Depending on content, I think it is often nice to have the option to transfer out to a call center agent since that role will never disappear. Some people prefer a human (look at all the grocery store lines) and some exceptions don’t fit into a rules-based decision tree.
It would have been more conversational for me to have talked with an automated phone call where I could answer questions with certain hotwords that dynamically moved me through the path of the call. Depending on content, I think it is often nice to have the option to transfer out to a call center agent since that role will never disappear. Some people prefer a human (look at all the grocery store lines) and some exceptions don’t fit into a rules-based decision tree.
But, quality is a huge issue with complex plan designs in healthcare. How do you teach each call center agent (especially when you have high turnover) to respond and explain things exactly the same? You can’t unless you force them to read a script which is a bad experience for the member / patient. We used to have to do lots of secret shopper calls to work with our agents to get them to the right place and meet minimum expectations. Again, this is something that a computerized system can address.
The thing I always hear about calls is aren’t they like those election calls I get where the voice sounds a little computer-like (aka text-to-speech) or there is a big pause between the person answering the phone and saying hello and the actual recording kicking in or the live person talking. With the top vendors out there, those are old issues. There is no pause. The messages are recorded in human voice. Ideally, the variable text (e.g., patient’s name or drug name) are part of a custom audio library which is in the same voice.
Avoiding Calls Then Texting
July 16, 2008 0 Comments
CNet has an interesting article about teens avoiding live calls only to text back the person immediately so they can continue their current activity. I do it all the time when I am in meetings or on conference calls.
They provide some interesting statistics on text messaging (see below) for this young group. Not a prime focus for healthcare, but it will be interesting to see how this use of technology applies as they grow older.
More broadly, nearly one out of every two U.S. tweens (or kids between 10 and 13 years old) and 83 percent of teens own a cell phone, according to new research from Chicago-based C&R Research. And with that many kids using mobile devices, the text messages are flying.
The average teen, according to C&R, generates between 50 and 70 text messages a day, or as many as 18,000 a year.
What Driving Teaches Us About Wellness
July 15, 2008 0 Comments
We all understand the challenges in getting people to take their healthcare seriously which manifests itself most prominently in a obese society which leads to numerous other conditions – heart disease, diabetes, high blood pressure.
I was reading an article earlier today about driving slower to maximize your fuel usage and thought what a great example of how people don’t do what’s best for them. You can reduce your fuel needs by driving slower, but most of us are too hurried to do that. We don’t follow practical, fact-based suggestions. It’s just like the challenges of eating well. It is much easier to go to the fast-food restaurant than to plan your lunch, buy healthy foods, pack a lunch and bring it to work.
 Another good link is between using a phone when driving and wellness. Again, we know that people being distracted by their conversations (voice and text) while driving can lead to accidents. Certainly, headsets and voice technology should reduce those distractions (although the data doesn’t support that). For example, when I am driving, I simply press the button on my Bluetooth headset, speak the person’s name, and then the phone calls them. Much less distracting for my eyes on the road…but I am still talking to someone and multi-tasking. So, again, why don’t we do what’s best for us and stay off the phone? It’s generally not efficient…we are pressed for time…we have become a country of multi-taskers. A similar reason to why lots of people don’t exercise…too busy.
Another good link is between using a phone when driving and wellness. Again, we know that people being distracted by their conversations (voice and text) while driving can lead to accidents. Certainly, headsets and voice technology should reduce those distractions (although the data doesn’t support that). For example, when I am driving, I simply press the button on my Bluetooth headset, speak the person’s name, and then the phone calls them. Much less distracting for my eyes on the road…but I am still talking to someone and multi-tasking. So, again, why don’t we do what’s best for us and stay off the phone? It’s generally not efficient…we are pressed for time…we have become a country of multi-taskers. A similar reason to why lots of people don’t exercise…too busy.
“There are limits to how much we can multi-task, and that combination of cellphone and driving exceeds the limits,” says David Strayer, a University of Utah psychologist who has found that by many measures, drivers yakking on cellphones are more dangerous behind the wheel than those who are drunk, whether the conversation is carried on by handset or headset.
Texting – We Are About To Call
July 15, 2008 0 Comments
I had one of our clients use an interesting banking example the other day. Initially, I was a little skeptical, but after an incident this morning, maybe there is a place.
They said their bank lets you opt-in to receive a text message right before they call you. It says something like “This is your bank. We are about to call you about your account.” Therefore, you are more likely to answer the 800# call you get on your mobile phone.
My immediate question is why doesn’t the 800# have a caller ID that shows who is calling. This can be a significant factor in getting people to answer the phone.
So, late Sunday night, I get a message from an 800#. I don’t listen to it until I get up at 4am this morning to catch a flight. Well, it was from American Airlines saying that they had cancelled my non-stop 6:45 flight and rescheduled me on a flight through Chicago that gets me there over 2 hours later. Since I have a 2-hour drive from that airport, I was a little panicked that I would miss a big presentation. I ran to the PC; found a new flight on Southwest that got me to a smaller, but closer airport; packed a bag since I was now going to spend the night; and went to the airport.
Had American texted me last night, I might have answered the phone and/or I would have read the text before crashing.
McKinsey On Automated Calling Technology
July 15, 2008 0 Comments
McKinsey and Company published a report called “Using IT To Boost Call Center Performance” in the Spring of 2006 which had a few relevant comments for those of you looking at how to leverage automated communications in the healthcare space. Here are the two primary quotes that I took away:
Customers are getting used to automated transactions – in fact, some prefer them. Our research suggests that more than 60 percent of customers favor an automated option for many types of simple interactions (for example, balance inquiries or payments); the rest said they didn’t mind being presented with an automated option as long as they could connect with a live agent if they wanted one.
Investments in new VR (voice recognition) and IVR (interactive voice recognition) technologies can help automate an additional 5 to 30 percent of incoming calls while maintaining or even enhancing customer satisfaction and revenue.
I always love finding those 3rd party verifications of the value propositions that we see at clients.
Medical Home
July 14, 2008 0 Comments
I just changed PCPs (primary care physicians) to find a new one who was easier to access and more personable. (Not that I had been to my other PCP in 5 years.) I was very pleased that this new individual has adopted the medical home concept. He wants to be my central point of contact, and he is a big prescriber of Ix (information therapy). It was interesting. Here are a few highlights from my introductory visit.
- His paperwork asks you to call him before going to the emergency room (ER) or urgent care.
- He does in-office dispensing using a company I know called Purkinje.
- He asks you to sign off on leaving you messages and/or who else he can talk to about your care if needed.
- Every time we talked about something, he would reach over and grab an article from a library on the office wall and give it to me to read.
- He gives you his e-mail for contact and talks about responding within 30 minutes.
Now, hopefully I don’t need much care, but I feel like I have found a good advocate and involved MD to work with. (He also came highly recommended by several people.)
IDC – Healthcare Communications
July 14, 2008 0 Comments
Janice Young at IDC just put out a new report titled “Too Much Information? The Irony of the Coming Information Glut and New Technologies that Help Target Communications” which focuses on several fast-follower announcements about what we have been doing at Silverlink Communications. Here are a couple of quotes from the report.
The final mile of the current healthcare information blitz is not just getting at or to the information, though in the very fragmented, silo’d U.S. healthcare system, that is hard enough. But the real solution provides targeted and event-triggered information based on consumer interactions or events, rather than relying on the consumers to search and seek.
These two announcements join Silverlink’s earlier announcement in March 2008 of their new Adaptive HealthComm Science Platform. The Silverlink platform integrates decision support and analytics to create personalized customer communications. Unique to the Silverlink solution are behavior analytics to communications success and affect on customer behavior and outcomes.
Beating The Patient Over The Head
July 14, 2008 1 Comment
Something that I don’t normally do, but I am going to edit this after the fact to stress what the story really is supposed to be about since someone told me the original text might be offensive to a competitor that I respect. The point is whether being pushy is worth it in some cases.
The other day a patient asked one of our people about a mail order order pharmacy where they had gotten a call every other day for the past 12 days about refilling their medication. Each message was slightly different – your supply of medication is about to run out, you need to refill your medication, your prescription has run out, etc. The patient didn’t like the call program.
I found this an interesting debate…how pushy is good if you drive a desired outcome? Also, we all obviously know that vendors and consultants don’t always make the decision so if a client tells you to do this even if it makes no sense, what do you do?
I think it makes for a good debate and had it with several clinical people:
- At what cost is a better refill rate okay…especially since this doesn’t mean that they are compliant? Are you willing to drop your patient satisfaction by several points? (We often used to give clients a report that showed savings per disrupted member or per drop in satisfaction at my prior employer.)
- If the company is just driving up refills and can they do that without creating more waste? This was a constant debate at mail. One trick here is whether you base it on refill dates or days supply.
- With this frequency of calls is there a chance that you actually get people that would have refilled to just wait for the calls to come and say yes?
- If people take the call because they know you will keep calling them, is this actually better acceptance of calls or just being an “obnoxious salesperson”?
- Are you calling people that have refilled at retail due to data latency issues?
- Do you drive people back to retail?
- Have you dulled them to future calls by upsetting them on this program?
Now, on a more clinical program, my opinion here might be different. If you could successfully get an overweight individual to diet by constantly reminding them. This might be okay. It’s an interesting debate.
One Year Blogging “Anniversary”
July 11, 2008 2 Comments
It was last July that I started this new blog originally called The Patient Advocate and now Patient Centric Healthcare. I pulled in some of the content from my old blog on Business Process Management (my focus during my non-compete days). I thought I would spend a minute and capture some statistics from this first year.
- 603 posts
- 272 comments
- Top posts:
- What is a PBM?, 2,880 views
- Zyrtec to Go OTC, 1,018 views
- Some Pharmacy Statistics, 1,014 views
- Total views – 43, 292
- Best single day – 379 views
- 116 subscribers – get a daily feed
- 13,377 spam comments caught (WOW)
It has been interesting to hear from and meet some of the readers. Additionally, I have enjoyed some of the opportunities it has created. I had a chance just the other day to do an analyst briefing on PBMs to one of the big investment firms on Wall Street.
And, one of my favorite things was that I got a signed book from George Halvorson the other day with a personal note about my comments on his book on my blog.
But, for all those that ask…it is a lot of work. I do it primarily because I enjoy it. I am not sure if these stats are just stats or indicate that it has been a successful effort.
Communication Chicken And Egg
July 9, 2008 2 Comments
You hear a lot these days about preference based marketing. The idea is that consumers (or members or patients) select how you interact with them. In healthcare, this means things like:
- What types of communications do you want to receive?
- How do you like to be communicated with – letter, web, live person, automated call, text message?
- When do you like to be communicated with – day, time?
 Of course, companies then have to figure out what rules to use in terms of when to trigger communications. The next question is how to personalize the communication.
Of course, companies then have to figure out what rules to use in terms of when to trigger communications. The next question is how to personalize the communication.
So an interesting question is…does the company have a responsibility to their members to use their data to drive them to actions that are in the member’s best interest?
Do companies always do what’s right…probably not, but I do believe that they want to do the right thing. They want to drive successful outcomes. They want patients to be healthy. They want patients to save money.
Now, my chicken and egg analogy is which comes first the selection of what my preferences are or experiencing the communication. How do I know whether I want a refill reminder if I have never received one? How do I know which channel I prefer if I haven’t experienced each of them? And, since each communication can vary based on messaging and many other variables, can one good or bad experience bias my selection?
Putting Your Kid On Cholesterol Drugs
July 7, 2008 4 Comments
I was a little surprised to see the news this morning claiming that it was okay to start putting kids as young as 8 years old on cholesterol lowering drugs and starting testing as early as 2 years old. Talk about an obesity epidemic out of control. I would think that there were lots of things we could be doing about diet and exercise to address this before setting kids up to be on these maintenance medications for the rest of their life.
Not a clinical opinion, but my personal opinion. It makes me think of the social commentary delivered in the new movie – Wall-e – where the people don’t know how to walk anymore and just float around getting fatter and fatter.
Medical Bankruptcies
July 2, 2008 1 Comment
I will give credit to the Health Care Reform Now blog for leading me to this article in The Indianapolis Star, but I think it is a sad reality.
“More and more of the middle class is finding out that even if they have jobs and insurance, they can be wiped out by medical events that are not even catastrophic,” says Dr. Christopher Stack, a retired orthopedist and co-founder of Hoosiers for a Commonsense Health Plan, the state’s chapter of Physicians for a National Health Program. “You can run up a high five-figure bill real easily.”
A Harvard study published in 2005 estimated that about half of all bankruptcies filed in the U.S. have their origins in medical costs, a ratio that jibes with Silver’s and other bankruptcy veterans’ observations here in Indianapolis. While the rest of the world’s industrialized nations provide health coverage to all or nearly all of their populations, the U.S. mass-produces the distinctly American phenomenon of medical bankruptcies.
I am not a big fan of the donut hole in Medicare, but perhaps we need a donut hole type concept for health insurance where people have a maximum out-of-pocket in any one year. Although I am sure that would beg the question of what was optional versus required surgeries and treatments. It just seems a shame that we can bankruptcy hard working people with insurance over their medical bills.
What is a Mail Order Pharmacy (Home Delivery Pharmacy)?
July 1, 2008 1 Comment
My most popular post ever is “What is a PBM?” which made me think that this is probably a relevant post for the average healthcare consumer. And, given the historical push to mail combined with the current economy, you can expect mail order pharmacy (or home delivery pharmacy) along with 90-day retail pharmacy to be a hotter topic.
At Silverlink Communications, we work with a lot of companies on their retail-to-mail (RTM) communications strategy and execution. One of the first things I point out to all of them is that over 50% of people don’t usually know what mail order pharmacy is. So, you have to address awareness at the same time as recruiting new patients.
So, for all of you that receive a letter or call talking to you about moving your prescription to mail order, let me answer a few of your basic questions:
- Mail order pharmacies are also called home delivery pharmacies since they deliver your medications through the mail and directly to your home (or other address provided).
- The mail order pharmacy is typically owned by either your managed care company (aka health insurer) or by a pharmacy benefit management company that your insurer contracts with directly to provide this service.
- There is typically only one mail order pharmacy that you can use (i.e., is considered “in-network”).
- The service is typically the fulfillment of 90-day prescriptions of medications which you will take on a long term basis (aka maintenance medications). This is not true for controlled substances which typically only allow a 30-day prescription and for some specialty and injectable drugs.
- You often have a financial incentive to choose mail order where you will get a 90-day supply for less than it would cost you to buy three 30-day prescriptions at your local pharmacy. This discount is due to the buying power of the mail pharmacy, the automation which reduces the costs of dispensing the drugs, and the lower distribution costs (i.e., no need to move the drug to all 5,000 retail locations).
- The drugs are the same drugs you buy at your local pharmacy.
- You have the same access to a pharmacist but it is over the phone not face to face (which I personally prefer and think is more confidential).
- You can do your refills over the IVR (interactive voice response) line and over the Internet along with traditional means of live agents and using snail mail.
- These mail order pharmacies use robotics and other highly sophisticated solutions to dispense the drugs accurately and quickly.
- Many of the mail order pharmacies that we work with offer services around calling your physician to get new prescriptions and also use our automated outbound calls to provide you with order status (WISMO calls – what is the status of my order) and refill reminders.
- You shouldn’t typically start a new drug at mail order. You want to wait until you have had two fills locally to make sure you are titrated to the right strength (i.e., your MD might switch your dosage initially so you don’t want to buy too much supply of a drug you might not use).
Are Involved Patients More Compliant?
July 1, 2008 2 Comments
This is a study from a few years ago from Harris Interactive and BCG that I found on the BioPlus website. If I am interpreting it right, it would imply that those that are most involved in their healthcare are most likely to be non-compliant. It doesn’t seem logical, but perhaps those are the people that want to play doctor and are most likely to think they know better.
Burning Calories – How Many?
July 1, 2008 0 Comments
I was with a friend and was talking about how many calories you burn per hour. The instructor at the aerobic kickboxing class I have gone to on and off for years always says that I could burn up to 800 calories per hour in the class. When I am on the treadmill, I always try to get it up close to 1,000 calories per hour. I have never been good about tracking calories in, but I always think about how much more I need to work out if I have been eating poorly.
So, if you’re looking for an estimators, here is a calculator and here is a great laundry list of activities from cooking to hiking and biking to broomball or calories burned per hour. I pulled a few common ones from their list here:
|
Activity (1 hour) |
130 lbs |
155 lbs |
190 lbs |
|
Biking (<10 mph) |
236 |
281 |
345 |
|
Biking (>20 mph) |
944 |
1126 |
1380 |
|
Golf (carrying clubs) |
325 |
387 |
474 |
|
Ice Hockey |
472 |
563 |
690 |
|
Pushing stroller with child |
148 |
176 |
216 |
|
Running (6 mph) |
590 |
704 |
863 |
|
Running (7 mph) |
679 |
809 |
992 |
Share This

My LinkedIn Profile

 WSJ Health Blog
WSJ Health Blog
- Is a Paleo Diet Healthier Than Standard Nutritional Guidelines?
- Small Business and the Affordable Care Act: How Has Your Business Been Affected?
- HealthCare.gov Explorer: Decode the Health Law’s Subsidies
- One Reporter, Four Families, Six Scientists and the Search to Cure a Rare Disease
- Your Responses: How Has the Health Law Affected You?
- What Does the Health Law Mean for You? Your Questions Answered
- How Has the Health Law Affected You?
- Rare Diseases and the Search for a Cure: A Reddit AMA
- Robots to Cure Rare Diseases: A Reddit Ask Me Anything (AMA)
- Six Tips For Better Napping
Drug Channels
- Drugs, Discounts and Data: Crafting Sustainability in an Imperfect System
- Drug Channels News Roundup, May 2026: My $0.02 on Optum Rx’s Transparency, Must-Read 340B History, PBM Unbundling Update, PA Delays, and Vegas Fun
- PBM Shakeout: How Vertical Integration Is Reshaping What’s Next (VIDEO)
- Protecting Gross-to-Net Performance Through Single-Channel Ecosystems
- Drug Channels News Roundup, Mid-May 2026: Flawed Launch Price Math, Rising Pharmacy Closures, Hospital Pay Realities, 340B Hospitals vs. Grantees, and a Luxury Take on Specialty Pharmacy
- 340B in 2026: Market Shifts, Policy Battles, and What They Mean for Stakeholders (NEW Live Video Webinar)
- The Hidden Costs of Over-Customizing Your Hub Technology Stack
- Specialty Pharmacy Accreditation: DCI’s Exclusive Analysis Reveals a Market at an Inflection Point
- Where Gross-to-net Pressure Actually Lives After Launch
- Drug Channels News Roundup, April 2026: PBM Specialty Pharmacy Steering, MLR Profit Shifting, Hospitals’ Fake Prices, and a Peek Behind the Scenes at DCI
KevinMD Blog
- An error has occurred; the feed is probably down. Try again later.
Health Populi
- What $37,824 Can Buy You in the U.S. in 2026: a VW SUV, a Year of College Tuition, or Healthcare for a Family of 4
- The Side Effects of Debt and Financial Stress Add Up to a Public Health Crisis in America
- Will AI Make Our Minds Feel Like Boiling Frogs, Be Borrowed, or Inspire Agency and Joy? Learning from John Nosta
- Will GLP-1s Shift the Actuarial Curves for Life Expectancy? Swiss Re Models the Scenarios
- The Blurring of Consumer Brands and Healthcare – HealthConsuming Goes Mainstream, Ipsos Reports
- The Cost of Confusion with U.S. Healthcare – a deja vu of The Temptations’ “Ball of Confusion”
- Gas ‘n Healthcare ‘n Groceries: U.S. Voters’ Cost-of-Living Concerns Will Inspire Them to Vote in the Midterms in the Latest KFF Health Tracking Poll
- Most Brands Speak to Women As If They Are Men: Learning from Hidden Women, Health Marketing Insights from 8th Day
- “Trust is the #1 Public Health Issue” and Health Citizens Live in an “Information Abundant” World That, Counterintuitively, Underpins Divisiveness – the 2026 Edelman Trust Barometer
- “The #1 longevity hack is ‘don’t be poor’” — Kara Swisher is a health economist
e-Patients
- SPM at the World Orphan Drug Conference
- Introducing the CHAMP Principal Investigator: Cait DesRoches (Part 2)
- Introducing the CHAMP Principal Investigator: Cait DesRoches (Part 1)
- Everylife Foundation Community Congress Annual Meeting Highlights
- Collaboration is the Best Medicine: Patient-Centered Collaboration Grounded in Caritas®
- Collaboration is the Best Medicine: It’s the Heart of Caregiving
- Collaboration is the Best Medicine: How to Partner with Your Doctor for Better Care
- Collaboration is the Best Medicine: Bridging the Gap in Patient Participation
- Dealing with Medical Uncertainty, Ambiguity, and Frustration
- Collaboration is the Best Medicine: The Time for Participatory Medicine is Now

Enabling Healthy Decisions Blog by www.georgevanantwerp.com is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 United States License.
