I was reading an article the other day about devices like FitBit and their use within corporate wellness programs. One of the questions it was asking was why use them when people abandon them after a while. I found this great chart from Endeavour Partners in their whitepaper which looks a lot like an adherence curve. They say that 1/3 of people abandon their devices within 6 months which makes it a hard investment for anyone.
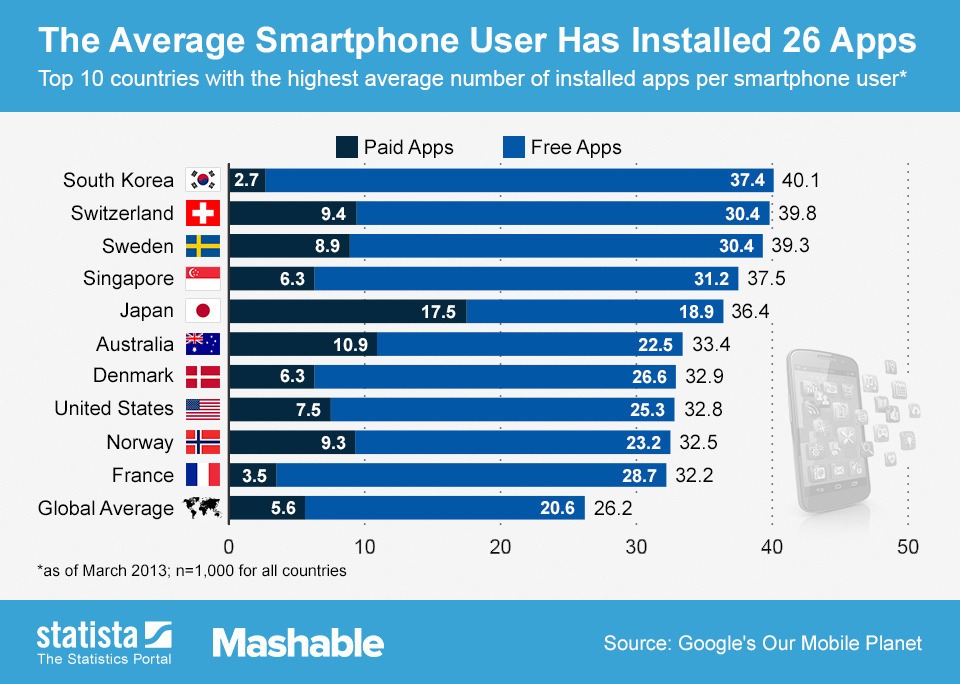
It’s the same question you might ask around mobile apps. While this chart shows that Americans install almost 33 apps, the questions is how long they use them.
According to Flurry, most apps peak within 3 months, and they show that health and fitness app retention is only 30% after 90-days. Again, that doesn’t make you want to invest a lot of money in a mobile app. But, there are lots of reports out there telling us that people want to use mobile to communicate with their providers, track calories, and do lots of other health related tasks. (see RuderFinn report, see IMS report, see Pew report)
So, what gives? Do we have unreasonable expectations? I would say yes.
We live in a ADD culture where people are constantly multi-tasking. People want things that evolve and constantly change. It’s the same reason we don’t want the same experience every single day. It’s the reason that you’ve seen people from gaming coming into healthcare. They understand how to keep people engaged over time.
Whether you want to picture it as a customer journey or different phases, the reality is that messaging needs to evolve with the consumer. If you got the same letter every month, at some point, you don’t even pay any attention to it. At some point, you wouldn’t even open it.
When I worked in healthcare communications, it was the same challenge from a strategy perspective. How would we coordinate communications across channels? What would the first message say versus the fifth message? How do you avoid message or channel fatigue?
It’s the same thing in the digital or device world. So, I ask the question…do we have unreasonable expectations about these tools by thinking that we can put them out there and sustain use of them? I think so. We need an evolving, constantly changing strategy about content, community, functionality, etc. to keep engagement sustained.
As I’m enjoying my time thinking about what’s next, one of the things that I’ve thought a lot about key problem areas in our healthcare system. Obviously obesity is one of them. And, you have lots of companies trying to figure out what to do here.
Build an assessment tool (like Milliman or InterQual) which could be used for assessing patients and creating an evidence-based care plan.
Work with KitchenAid or others to create a branded line of smart devices which used the Internet of Things to do things like re-order healthy foods and suggest menus.
Work with FitBit or other device company and a gamification company to create a kid’s device linked to a game where the key player got fat tied to their activity level and where they opened up new levels tied to their behavior (e.g., eating healthy).
Create online communities for people to share stories and experiences (like PatientsLikeMe but moderated).
Work with Healthways and the Blue Zones effort to create a family centric option tied into the schools and focused on getting everyone healthy across generations.
Create a mobile coach using embodied conversational agents (similar to avatars) to drive behavior change and create a location-based prompts (i.e., as I pull into McDonalds).
Work with manufacturers to create a “beyond the pill” approach to obesity drugs that incorporates coaching and behavior change with the pill being the final mile which should drive greater formulary coverage.
Create a detailed patient journey map based on ethnographic research for weight loss with different triggers and create a “Coach certification” that can be used with coaches to certify that they are following best practices.
Work with biometrics companies (e.g., LabCorp, Quest) or clinics (e.g., MinuteClinic) to create an early identification process for obesity and/or metabolic syndrome with a process for them to “prescribe” a specific program.
Research and design ethnic specific obesity related programs for sub-populations within the US. For example, partner with the large Hispanic groups to create a Spanish (language, experience, culturally relevant) programs.
Partner with the ADA and NKF to jointly address metabolic syndrome together.
Work with a grocery store or food company to create an augmented reality process for smart phones or Google Glass that would highlight healthy foods on the shelf and help people shop better.
Work with Medicaid to create a process by which people earned cell phone minutes or lower copays based on activity and participation.
You can see companies building innovation teams and innovation labs within healthcare. You see lots of new entrants trying to figure out how contribute in this space (e.g., Qualcomm Life). But, some of these just become ivory towers where they pontificate and put out cool ideas. Others disappear because they can never be commercialized. Others fall into the “fast fail” bucket of companies, and only a portion of those actually innovate well.
This is a nice report, but it’s a little too high level for me. It has some great frameworks about what to do and some nice graphics, but it’s not operationally practical (although that may not have been the purpose). Here’s a few things I highlighted:
“Mobile Health – The use of mobile applications and devices to deliver medical information, access or record data, or provide clinical services – has the potential to revolutionize patient care.” [good definition]
“The gap between the current market size and five-year projections is significant.” [so is it a warranted gap or will it get closed…I think it will be a challenge to meet expectations.]
They hold out 3 barriers – entrenched behaviors, reluctance to pay, and fragmented infrastructure. [I would agree but how do I work through these…they provide some thoughts.]
They talk about creating a “must-have app” that would consolidate multiple offerings into a single solution. [I don’t even think this silver bullet approach should be considered…It won’t happen.]
They seem to fall into the traditional trap that people other than the payers and employers will fund these programs (telcos, pharma, device companies). [Everyone wants that, but I think that’s the wrong framework.]
They talk about an option of creating and charging a premium for mHealth offerings because some of them “deliver objectively better outcomes or lower costs compared with traditional health-care offerings”. [Really? That’s great news, but I wouldn’t consider that a fact. I’d say we’re seeing some promising studies.]
They talk about “an orchestrated ecosystem” and integration of data. [This would have been a perfect time to highlight what Vladic is doing or what Dossia is doing.]
There were some things missing that I personally would have called out.
What about learnings from prior models like electronic prescribing?
What about things like EMR integration and the difficulties there?
What about the issue of privacy and security?
What about the fact that people abandon devices and apps very quickly?
What about learnings from gamification or incentive management?
What about prescribing apps to patients? (like Happtique or IMS)
It starts with a great tag line from IBM – “Does Your Kid Have Better Technology Than Your Business?” They reference Steve Case’s framework from a presentation he made (see below):
What I liked about this report is that it’s based on lots of real world examples. (It’s still not operationally helpful, but these are investors not consultants so it met my expectation.) They certainly could have gone deeper to explain why certain companies they highlight got acquired such as Diversinet, Epocrates, BodyMedia, CardioCom, Healthagen, Vitality, and ConsultADoc. But, if I look at their list of companies, I see a lot of the innovative companies that I would have on my list – Proteus Digital Health, Healthrageous, iTriage, TelaDoc, Telcare, Eviti, Change Healthcare, and Asthmapolis. (I know Healthrageous shut down – see postmortem – but I think they had some great vision.)
I also think they’re list of major inhibitors to growth was very believable:
Physician adoption
ROI
Regulatory hurdles
Security and governance
Lack of standards
The report shares an interesting stat that 45% of the companies that applied for their rewards were led by MDs in 2009 while it’s only 21% now. To me that shows the movement of IT and business executives into the healthcare space.
Triple Tree does talk about remote monitoring and CMS which I think is important. While the Veteran’s Administration was mentioned in the BCG report, I think that the government efforts here and influence was generally overlooked.
Overall, two interesting reports. Worth a read although I would choose the Triple Tree report over the BCG one if I had time to only read one.
Two other places that I would recommend going if this topic is interesting are:
I try not to do a lot of promotion of things within the company. (This is not a corporate blog.) But, I’m always happy to share cool things that are in the public domain that catch my eye.
I’m always thinking about different ways to blend companies through acquisitions or partnerships. The announcement by NantHealth the other day at HIMSS got me thinking more about it. They are an interesting company from what I can tell although I don’t know anyone there.
I’ve talked about Google and all their health assets although they’re not actively trying to integrate them. I also think that there are some investment firms like Sandbox Industries that have their fingers in lots of interesting healthcare companies.
So, what would some other interesting opportunities (M&A, partnership, JV) be (ignoring size, valuation, ownership, and likelihood):
Eviti and Best Doctors (expanded Oncology footprint) and then perhaps a pharma or specialty PBM
Ceridian and Ginger.io and Cogito (behavioral health) and then perhaps a outsourced call center company
Of course, I’ve talked about different PBM plays recently, and I think healthcare has become such a front page issue that companies like McKesson, GE, AT&T, Emdeon, Cisco, Apple, and others are waiting to figure out how and when to buy up some technology plays. I could easily see McKesson jumping in to buy several of the adherence companies that I highlighted a few weeks ago like Proteus. And, I’m sure there’s more from this list of fastest growing healthcare companies that will get snapped up or create some interesting partnerships.
I also believe that health reform will drive some consolidation on the provider and payer side. A friend on Wall Street predicted we’d get to 6 national health insurers. I still think that’s possible – United, Aetna/Cigna, Wellpoint/BCBS, Kaiser, Humana, and ??
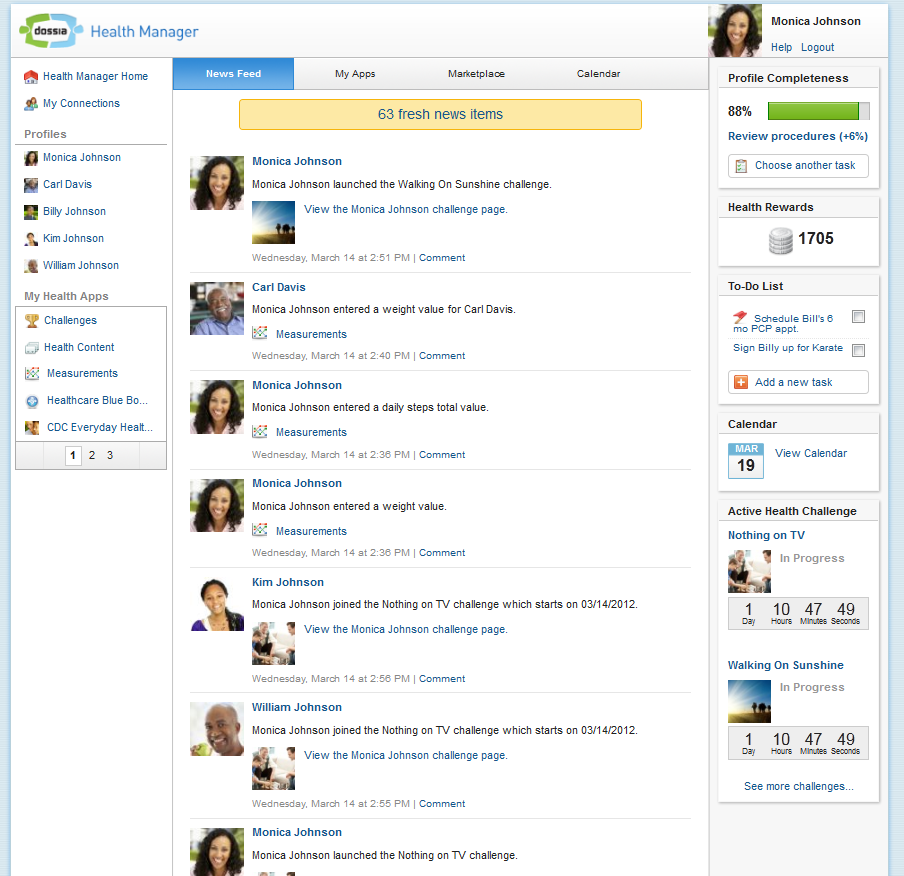
I had a chance to see a product demo of Dossia the other day. I was really impressed which I don’t easily say. I was expecting to hear a pitch on Personal Health Records (PHRs) and why they were different. Instead, I got to see a robust patient engagement portal which did some really interesting things. (see image above from the Health 2.0 demo they gave)
From their website, here’s the “about” description which lists some very influential players…
Dossia is an organization dedicated to improving health and healthcare in America by empowering individuals to make good health decisions and become more discerning healthcare consumers. Backed by some of the largest, most respected brands in the world – Applied Materials, AT&T, BP, Cardinal Health, Intel, Pitney Bowes, Vanguard Health Systems, NantWorks and Walmart – Dossia’s founding member companies have united under the common vision of changing healthcare.
Having these companies involved over the past 6 years has been really important for them to accomplish what they’ve done. As someone that’s worked on a lot of the same population health challenges, they’ve accomplished things that not even Google Health could do.
So what were the features and functions that really impressed me:
They’ve built integration to health plans, PBMs, pharmacies, lab companies, and even EMR companies. This creates a data rich longitudinal view of the patient for the patient. (I like the expression on their website where they say “Dossia is the connective tissue that powers healthy change.”)
They’ve incorporated health content which by itself isn’t impressive, but the content is tailored to the individual based on their medical data. Not hard, but not something that many people do well.
They’ve built out a series of partnerships and integrations with over 50 apps where you can navigate that turn them on as widgets within the portal. This is very similar to some of the cool things that CarePass is doing.
They’ve built the system out using open APIs (application programming interfaces) which allows other companies to easily integrate with them.
And, probably one of the cooler things from my consumer engagement lens was their ability to do WYSIWYG rules creation to trigger outbound communications based on clinical data. The idea of a rules engine isn’t difficult, but the ease of their solution with the integrated data makes it very powerful.
And, they’ve expanded their reporting. They’ve pulled in ways to manage those family members for which you’re a caregiver. They’re doing lots of interesting things. They are definitely worth talking to if you haven’t seen them in a few years.
Google Health was a personal health information centralization service (sometimes known as personal health record services) by Google introduced in 2008 and cancelled in 2011. The service allowed Google users to volunteer their health records – either manually or by logging into their accounts at partnered health services providers – into the Google Health system, thereby merging potentially separate health records into one centralized Google Health profile.
And, I would also point to the intelligent home (per their acquisition of Nest) as a venture which will lead them down the path of health at some point.
You could also look at the companies that Google Ventures is investing in from the health space:
I could have easily seen them investing in something like Theranos which stands to change the biometrics space.
So…it’s not like they’re ignoring the space which isn’t unusual for many companies outside of healthcare. Healthcare is hard. Healthcare has lots of regulatory constraints. In general, many companies want to avoid having to deal with some of those issues which can constrain the rest of their businesses.
But, let’s look at the critical and hot topics in healthcare right now:
BigData – how to use data; how to build predictive models
Engagement – how to personalize communications and engage consumers to take action from mass customization to segmentation to even gamification
Social – how to use social pressures and peers to create better health
Connectivity – how to connect devices, caregivers, pharmacies, providers, and others into a shared platform for care
Security – how to securely manage data
Transparency – collecting and aggregating pricing data to help consumers make intelligent decisions
User experience – creating user journeys and user interfaces to improve the overall consumer experience (perhaps changing the model like Uber (a Google Ventures investment))
Do those things sound like the competencies of any one company? To me, they all sound like things that Google is good maybe even great at. Additionally, the founders of Google have the big, picture and long-term vision that’s critical in healthcare. Driving change in healthcare isn’t about meeting specific quarterly numbers. It’s about seeing the world in a new light where you want to drive change and improve things like childhood obesity. It doesn’t happen overnight.
I wish I knew more about Google. Someday, I’d love to work with them on some of these opportunities. If so, I could see this being a perfect fit in the Google X world. I could see them making a change as a core focus, as investors, or simply by creating enabling tools. But, at the end of the day, this is why I think health needs Google to have a focus here. It’s almost 20% of our GDP and something that impacts most people on a daily basis.
By now, the idea of a PBM and who they are is much more of a household item than it was a decade ago. We’ve seen massive consolidation in the industry. We’ve seen PBMs grow in the specialty PBM space. The question I often ponder is what’s next. Here’s some of my thoughts.
Do Nothing. Obviously, there’s a lot to be said for ongoing momentum. The PBMs have shown growth for many years. While the generic opportunity and the mail opportunity has slowed down, there are still opportunities in the specialty space.
Distribution. This seems like an obvious possibility. Why not buy Cardinal, AmerisourceBergen, or someone else? Procurement and distribution are core competencies so I think this makes some sense. But, will that create issues in the current client list and retail pharmacies and PBMs haven’t always had the best relationships. (E.g., Express Scripts GPO with Kroger)
Pharma. This has been debated by a few PBMs, but getting into the R&D space is risky and doesn’t build on their core competencies. What could be more interesting would be them getting into the services space by acquiring a company like IMS or Quintiles.
International. Several PBMs have tried this model. In general, it hasn’t gone anywhere. I think the international collaboration of Walgreens and Boots is really interesting and other retailers have gone international. I don’t see this happening anytime soon with any material impact.
Physician. Having a greater impact in the prescribing process could make a lot of sense. I could see some interesting targets in terms of Allscripts, Cerner, or athenahealth. This has been a challenge for years with a few ventures into the space. (e.g., CVS Caremark and iScribe)
Technology. At the end of the day, the PBMs are large technology companies. Could they see their way into the mHealth space? This space is growing like crazy, and you’re seeing established players get into the remote patient monitoring space (e.g., AT&T and Qualcomm). I could see an acquisition in this area of a telehealth company (e.g., Teladoc) or a device company (e.g., Welldoc). Or, they could build something more organically. On the flipside, they could look at technology platforms to open doors to care management or ACOs (e.g., Lumeris). Alternative, I could see SoloHealth as a really interesting asset.
Retail. With a few exceptions, I think this strategy is off the table. I’ve loved the CVS Caremark integration for years, and I think it’s showing dividends. Rite-Aid is probably the only big acquisition target out there. In this space, you probably have to look at it the other way. Would any retailers (e.g., Walmart, Walgreens, Target) buy a PBM? Walgreens got rid of their PBM, and Walmart has said they don’t want to be in that market so I’m not sure that would go anywhere.
Insurer. I think this one has some interesting opportunities from a Medicare perspective and from a commercial perspective. Could PBMs create an underwritten product and take on risk? I think yes, BUT I think that could impact their need for reserves and the way the market sees them. That makes me think this is less likely, but possible.
Device Benefit Management. I think several ex-PBM executives have gone out to try to build the “benefit management” concept into the healthcare marketplace in other areas (e.g., IPG). Could an existing PBM do it and cross-sell into their base? Perhaps. But, a stretch. They’re getting big so they want to buy meaningful revenue, create synergies, and then grow it.
Navigation. The most used benefit is pharmacy. Today, consumers touch the healthcare system most frequently through retail and their daily prescriptions. With the ongoing complication of the health benefits, there is a huge need for navigators (and not just in the healthcare.gov use of the term). Think about companies like Health Advocate or Accolade.
Data. With the RxAnte acquisition, it has to make you wonder about PBMs and their data assets. How can they use them differently? Can they create apps? Can they create algorithms to license? What would this look like? What about companies like Proteus? Perhaps, a PBM could consolidate several unique assets along the device, smart bottle, data path.
Condition specific. I could see some PBMs going deep on particular areas like oncology to really build out an oncology practice that did everything from second opinions to case management to end-of-life counseling. Those could all wrap around the drugs. Or, imagine them going into the chronic kidney care space by acquiring a company like DaVita.
Providers. While there could be some interesting synergies here with a large hospital group (e.g., HCA) or some ACO/PCMH players, I see that more of a managed care play for rolling up companies. The ROIC (Return on Invested Capital) is too different in these physical operations that I see that being a struggle. And, I think there’s lots of concerns about the hospital needs over time.
Which path plays out…I don’t know, but I think it’s getting close to time that you’ll see another shift in the market as they try to secure their next 10 years of growth by expanding into something that builds on their core competencies.
I think the other question would be if they focus on differentiation by really showing material differences in outcomes and engagement rates and look at how they show an overall health ROI not just Rx specific. That would be where I would place my bets and look at which of these options support that. Maybe we’ll see a PBM X (like Google X) doing some strategic long-term deals to change the overall healthcare roadmap.
In 1998, I wrote my first business plan which was about technology and architecture. At the time, I had graduated from Architecture school and was working with Sprint on a data warehousing implementation. It got me thinking about how to create a series of connected devices and link them to an enterprise system to manage that data for a smart home. At the time, I think people thought I was crazy.
Jump forward 15 years and it all seems to make more sense. For example:
You have remote patient monitoring solutions like Healthsense working on smart beds, toilets, and other sensors that track motion and other activities in the home.
You have smart pill bottles. You have smart pills with companies like Proteus Digital Health.
“The Internet of Things (or IoT for short) refers to uniquely identifiable objects and their virtual representations in an Internet-like structure. The term Internet of Things was proposed by Kevin Ashton in 2009.[1] The concept of the Internet of Things first became popular through the Auto-ID Center at MIT and related market analysis publications.[2] Radio-frequency identification (RFID) was seen as a prerequisite for the Internet of Things in the early days. If all objects and people in daily life were equipped with identifiers, they could be managed and inventoried by computers.[3][4] Besides using RFID, the tagging of things may be achieved through such technologies as near field communication, barcodes, QR codes and digital watermarking.[5][6]
Equipping all objects in the world with minuscule identifying devices or machine-readable identifiers could transform daily life.[7][8] For instance, business may no longer run out of stock or generate waste products, as involved parties would know which products are required and consumed.[8] A person’s ability to interact with objects could be altered remotely based on immediate or present needs, in accordance with existing end-user agreements.[3]
According to Gartner there will be nearly 26 billion devices on the Internet of Things by 2020.[9] According to ABI Research more than 30 billion devices will be wirelessly connected to the Internet of Things (Internet of Everything) by 2020.[10] Cisco created a dynamic “connections counter” to track the estimated number of connected things from July 2013 until July 2020 (methodology included).[11] This concept, where devices connect to the internet/web via low power radio is the most active research area in IoT.”
“More objects are becoming embedded with sensors and gaining the ability to communicate. The resulting information networks promise to create new business models, improve business processes, and reduce costs and risks.”
Of course, the key is a core infrastructure that manages all of this data and starts to create algorithms for how to use it. Image being able to log in and get information about your house, your kids, your community, and your health. Some things are already out there and being developed.
Mother is a technology that summarizes all of this data and pulls it together for people to use and monitor.
Twine monitors your home and provides you with information such as your garage door is left open.
Ninja Sphere is another solution for controlling your home devices.
Thing Worx is another solution focused on this connected house.
Qualcomm and Verizon and others are getting into the health space, and you have companies like ADT or Time Warner that are already in the home and could expand into the health space.
The other thing that all this data drives is the need for insights. It’s no good to have data without the ability to turn it into knowledge. This is again something that Google knows a lot about. Imagine having a connected team of physicians that monitor your health based on your sleep patterns, your adherence, your exercise, and other key metrics such as blood pressure. Imagine a dietician that monitored your food and gave you ideas about how to eat better. There are lots of ways for the data to be used in an obviously Big Brother way, but if that could be turned on and off, then we could gain the insights without having to give up all our privacy.
But, in general, many people are willing to trade privacy for insights. That’s what we do every day.
This idea of the Smart Home or Connected Home or Intelligent Home got me thinking over the holidays. I even emailed Pulte Homes and Lennar Homes to see if they were doing anything in this space. (They didn’t respond.) I did stumble upon Home For Life Solutions which seems to be thinking about some of this and was talking about this back in 2009 in an article about Smart Homes and Aging in Place. I was talking to a friend on Friday, and he shared with me some very cool things that The Villages in Florida is doing to incorporate health into their community.
I can see so many opportunities here especially around the concept of Aging in Place. Imagine all the Baby Boomers getting older and wanting to stay in their homes. I’m not sure what Calico is going to do, but this could be an opportunity for them.
In a recent issue of TIME, Page discussed how Calico will treat aging and related diseases. He didn’t reveal much about the methodology, but stressed that Calico’s team will “shoot for the things that are really, really important.” The goal for Calico’s research according to Page, is to help prevent many diseases and have a greater impact on public health than drugs that target individual diseases. (from MedCity News)
Imagine if this community existed. You would be able to create your own insurance company. You could offer discounts. You could do the same with life insurance. It could be like the Snapshot from Progressive.
And, there is so much more opportunity:
When you drive into your driveway, why can’t your garage door recognize you. Why do you have to press a button to open the garage?
Why can’t my purchases at the store be tracked online so I always know what I have and what I need?
Why can’t a smart cookbook recommend a recipe for tonight based on what food is at home, what food’s about to expire, and what I ate for lunch to create a balanced menu and caloric mix?
Why can’t my devices order my prescriptions for me when I’m low?
Why can’t my calendar automatically reschedule my doctor’s appointment when something else comes up?
Why can’t my running shoes automatically order a new pair of shoes when the cushioning gets low due to too many miles?
One day, this will all happen where our house will be smart. It will understand what I like in terms of lighting, shows, and music. It will tap into my devices. And, I’ll be able to get monitored and insights that improve my life. And, best of all, this will be done in a sustainable way that improves the environment and our quality of life.
So…maybe I can get Google or someone else excited about this idea! It will take someone with a big vision to change the world, but I think it’s a huge opportunity!
David is a founding partner at Janssen Healthcare Innovation where he is part of a multi-disciplinary group working toward the goal of propelling the company to become the leader in the healthcare solution business. Prior to the launch of the JHI team, David was with Johnson & Johnson for over 15 years.
“Janssen Healthcare Innovation (JHI), an entrepreneurial group within Janssen Research & Development, LLC, develops cutting-edge health solutions designed to modernize healthcare delivery, improve patient outcomes, and create a healthier world.” This is a 3-year old effort by Johnson & Johnson focused on integrated care businesses and enabling technologies. To support those, medication adherence and mobile are key areas.
One thing that David stressed is that they are platform agnostic and that their Care4Today Mobile Health Manager works as both an app and via SMS. Therefore, the 50% of the US that doesn’t have a smartphone can still use it. Additionally, it’s not a product or drug specific solution. You can use this even if you don’t use a J&J product.
Adherence is a huge challenge that everyone is aligned around, and everyone is trying to find solutions – plan design, incentives, apps, consumer engagement, framing, behavioral economics, and smart pill bottles (to name a few). So, what’s part of the Care4Today solution?
It has reminders for Rx and OTC products.
It has a refill reminder process which they hope to automate in the future.
It has a two way secure messaging platform.
It has images of over 20,000 pills.
And, they also included a caregiver strategy and an incentive option.
The idea of social health is important. We’ve talked about this for weight loss and smoking. But, with the expanded role of caregivers, can they play a key role in improving adherence? For example, if you respond that you didn’t take your pill and the response goes to your caregiver, will they call you? Will that follow-up motivate you? (Care4Family) Some prior research says yes.
A broader question might be about how to pick a caregiver or how to define it. Should it just be your family? Should it include your physician? What if you don’t have a support system? Could the healthcare companies or advocacy companies give you a “professional caregiver”? What about an avatar as a caregiver?
I asked about the incentive program that they included (Care4Charity). David pointed out that using apps isn’t fun (at least for most people) so they wanted to give a slight motivation. I questioned him on why $0.05 (which is the daily donation if you check in and take your meds). They did lots of research which showed that the amount didn’t really matter. So, this is an experiment to see if this extra feature of the program will nudge people to be more adherent. Or ultimately, it would be great to segment the population to understand who it was motivating for and for whom it didn’t matter.
One of the things I wondered about was how they were going to promote the app. Obviously, relationships with companies like Aetna and their CarePass program are one way, but with the tens of thousands of apps out there, how will people find it? David told me that they were going to initially focus on social media – Facebook, Twitter, and mommy blogs – to drive awareness. Next, they’re going to use pharma reps to discuss the app with physicians and pilot this strategy in HIV.
At the time, they’d had over 55,000 consumer downloads, and they’ve already gotten some initial feedback from physicians that like the fact that they’re offering solutions that aren’t branded to a specific pharmaceutical product. Some of those physicians are already offering it to patients. They expect this will be a big driver. They are now starting to talk with retail pharmacies about how to encourage consumer use. While my initial reaction was that this would be “competitive” with the Walgreens and CVS Caremark mobile solutions, they see collaboration opportunities especially with Walgreens and their open API.
Of course, I wondered about how the app was being used, but they don’t collect PII (personally identifiable information). In the future, they plan to offer an option for patients to opt-in to share information and create a clinic dashboard for physicians to see which patients are using it and providing them with data. And, with a new collaboration with HealthNet, consumers will be logging into the app with their HealthNet ID which will allow them to link up PII and PHI (protected health information).
So, what’s next…
They’ve launched in the US and France. They’re expanding into the UK and other countries next.
They’re adding Spanish in Q1-2014.
They’ve just completed some human factor testing which will drive some UI and UX changes.
They’re going to do some testing and look at results with whatever data is available.
They’re going to try to partner with as many people as possible.
Will it move the needle around adherence? It’s still too early to tell. But, it’s great to see pharma testing new strategies and working in new ways with payers to try to address this challenge.
A few weeks ago, I had a chance to follow-up with Martha Wofford, the VP of CarePass about their latest press release. This was a quick follow-up interview to our original discussion. As a reminder, CarePass is Aetna’s consumer facing solution (not just for individuals who they insure) which integrates mHealth tools and data to help consumers improve their engagement and ultimately health outcomes.
“Many Americans have a lower quality of life and experience preventable health issues, adding billions of dollars to the health care system, because people do not take their prescribed medications. There are a myriad of reasons why medication adherence is low and we believe removing barriers and making it easier for consumers to take their medications is important,” said Martha L. Wofford, vice president and head of CarePass from Aetna. “As we continue to add new areas to CarePass around medication adherence and stress, we seek to provide people tools to manage their whole health and hopefully help people shift from thinking about health care to taking care of their health.” (from press release)
As part of this update, we talked about one of my favorite topics – medication adherence. Obviously, this is a global problem with lots of people trying to move the needle. In this case, they’ve included the Care4Today app from Janssen. This tool does include some functionality for the caregiver which is important. It also links in charitable contributions as a form of motivation. We talked about the reality that adherence is really complex, and people are different. This may work for some, but adherence can vary by individual, by condition, and by medication. But, they hope that this is a tool that may work to nudge some people.
I was also glad to see them taking on the issue of stress by adding the meQ app. This is a key struggle, and Martha pointed out to me that 1/4 of adults are either stressed or highly stressed.
“When people are under chronic stress, they tend to smoke, drink, use drugs and overeat to help cope. These behaviors trigger a biological cascade that helps prevent depression, but they also contribute to a host of physical problems that eventually contribute to early death…” – Rick Nauert, PhD for National Institute of Mental Health, 5/2010
She mentioned that they’ve gotten a great reception to this program, but they have a lot more to learn. They’re still in the early period of getting insights and interconnecting all of their efforts. We also talked about some of the upcoming opportunities with the caregivers (or the sandwhich generation). I personally think the opportunity to improve aging in place through a smart home strategy with remote monitoring is going to be huge of the next 10 years.
I did interview the Janssen people as a follow-up which I’ll post separately, but I also thought I’d include this video interview of Martha that I found.
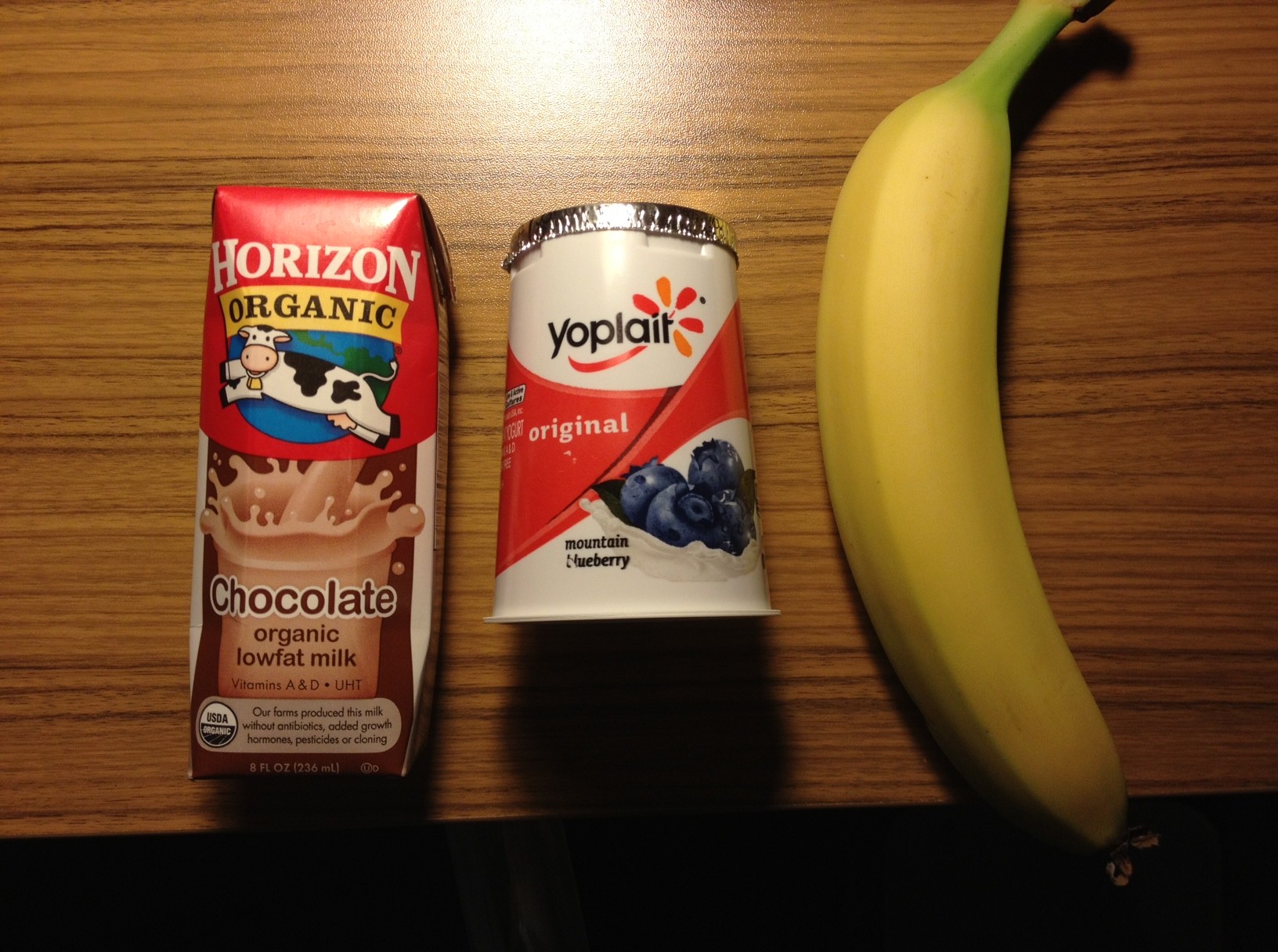
I’ll admit that several people have asked me about this over the years. If a picture is really worth a thousand words, would it be better to send someone a picture than a text message. Perhaps a picture of me in my skinny jeans if I’m trying to lose weight. Perhaps a picture of my grandkid if I’m trying to get healthy to run around the yard with them. Perhaps a picture of my favorite vacation location to motivate me to stick with a health goal. It’s an interesting question.
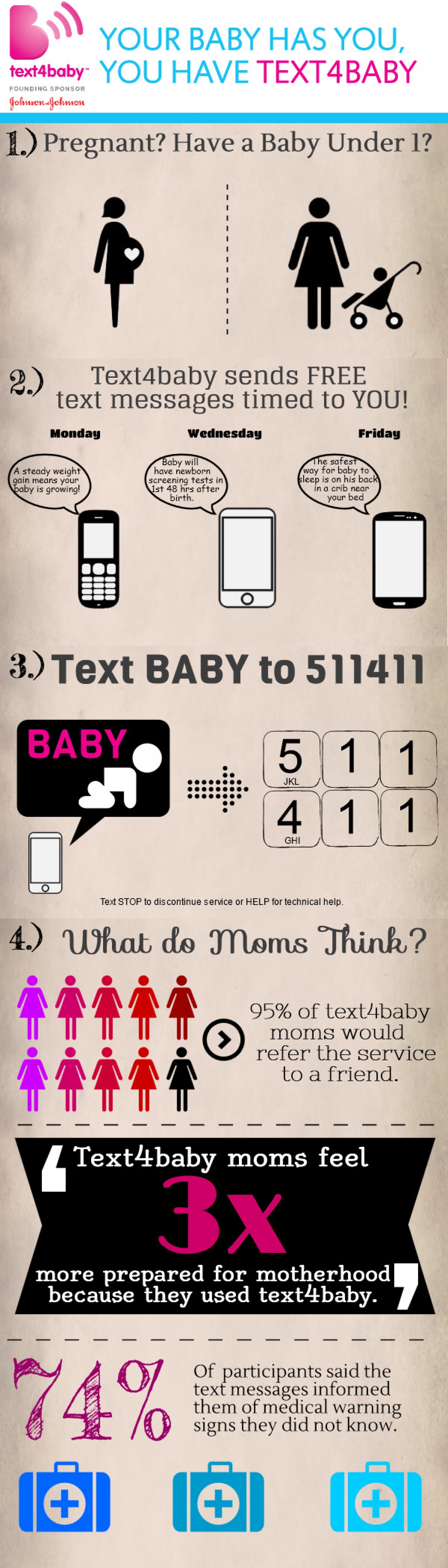
So, let’s start with tex messaging in healthcare. When I think of using SMS (or texting) in healthcare, my first example is always Text4Baby which was a unique coalition of companies that worked with Voxiva to get this launched.
Of course, Voxiva has since expanded to offer other programs:
And, I think there are some business cases out there around using SMS to interact and change behavior in healthcare. The Center For Connected Health in Boston with Dr. Joseph Kvedar has been studying this in several settings. Here’s one poster from them on a pilot. Here’s a good summary of what had happened as of 2012 from MobiHealth News.
I could go on, but I think you get the point. Lots of people have tried using text messaging as a low-cost but potentially effective way to get messages to consumers about a specific health behavior. Especially in other countries, this can be the preferred method.
I was thinking about my interview with Aetna about CarePass and what CarePass was doing, and it seemed to create a good example. Would I rather a text that reminded me about my goal or the picture on the right?
Additionally, I know in discussions with Vic Strecher, co-founder of HealthMedia, that we’re talked about the value of customizing imagery on letters to personalize and engage consumers. I just can’t find anything published by them right now to show that they studied that.
So, as we think about motivating people and sending them reminders, I think it would be really interesting to see the results of a picture driven process versus a written communication. Is it the same effect? Does it vary? By age, gender, type of action? Of course, the one thing I would recommend is letting the consumer upload and pick their picture not picking from some general list of canned photos.
Happy New Year! 2013 has been an interesting year in healthcare with 2014 promising many more exciting developments. A few of the biggest stories from 2013 include:
Healthcare.gov – the politics, the drama, and the missteps
Healthcare transparency and costs – new companies, new revelations, and an entire Time magazine focused on it
Healthcare engagement – ongoing focus on how to get consumers to engage
mHealth and QuantifiedSelf – apps and devices proliferate
Investment – a huge jump in VC and angel funding for healthcare
ACOs – do they work or not
Big Data – so much data…so many opportunities
Here’s my predictions for 2014:
Transparency – The race to bring cost data to the forefront of the consumer mindset will move from a radical concept to an expectation. With increased out-of-pocket costs and HDHPs, consumers will expect access and information to cost data. They will look for systems that can predict what they need and push data to them in a timely fashion using location based services and predictive algorithms.
Exchanges – With big companies trying the private exchanges and moving their employees to the federal exchange, we’ll see the market holding its breadth to see what happens. If this drives success on both sides of the equation – employers and payers, you can expect a large jump in this direction later in the year.
Mobile – The traditional member website will continue to die a slow death without mobile optimization in place. More and more consumers will access the healthcare system through a smart phone or device like an iPad. This will drive healthcare companies to figure out how to embrace user design and member experience in new ways as they strive to provide the sustainable app that consumers use more than a few times.
Providers – Providers will continue to cautiously embrace pay-for-performance, value-based healthcare, and models like ACOs and PCMHs. They will want them to work, but they will continue to look for the Tipping Point in which their overall panel is part of these programs. Providers will also begin to modify their workflows using technology based on Meaningful Use and the ubiquity of technology.
Engagement – Consumer engagement in healthcare will continue to be the elusive Holy Grail. Companies will try behavioral economics, incentives, and mass personalization to try and get consumers to understand healthcare and take actions to improve their health. There will be more shifting to include caregivers and embrace social media (e.g., Facebook) and peer-to-peer networks. We will start to see documented case studies and results in terms of improved outcomes.
Devices – While 2013 was the year of device proliferation, we will see the number of people (early adopters and QuantifiedSelf groupies) maxing out. I expect some further consolidation and a dip in adoption rate as we move into the period of disillusionment. Devices will be less about a standalone solution and look at how they integrate with the smart phone and existing systems (at work and home). Like smart pills and smart clothes, this will lead to increased data and integration into daily life. This will require collaboration with providers and employers to figure out how to come through this period.
Value-based – CMS will continue to be a big driver in pushing new payment models around healthcare as they struggle to figure out how to slow the tidal wave of costs coming in Medicare and Medicaid. This will meet up with some of the progress in the commercial space with ACO and PCMH models leading to an evolving path in terms of how drive value. This won’t be the breakthrough year, but we’ll see meaningful progress.
Investments – I don’t see any slowdown in healthcare investments. Our health issues aren’t going away in the US or abroad. China is just emerging with a long list of health issues and technology is creating new solutions in 3rd World countries.
Pills Plus – With pharma struggling with how to reinvent itself, they are going to look at new solutions like Merck is doing with Vree Health. This will cause them to look at many of these trends and how they wrap services, technology, and incentives around their medications.
Specialty Care – Specialty pharmacy will continue to be a big growth driver with novel innovations coming down the pipe. But, these pharmacies will realize that they can’t work in a vacuum. They have to do a better job at integrating care management into their services and partnering with Case Management companies to holistically treat the patient.
Metabolic Syndrome – The overall global issues of obesity and diabetes will become a huge weight around the shoulders of the healthcare system. While the focus will continue to be on the complex cases requiring massive dollars, the majority of people will be struggling with a chronic disease. Metabolic Syndrome will become a big focus for payers, employers, and health services companies as they try to find ways to prevent further complications.
Prevention – While I don’t expect a huge shift here, I think we’ll start to hear more voices on the perimeter yelling about why we only spend 5% of our dollars on prevention. They’ll point out other models outside the US spending more with better outcomes. Health Reform will begin to enable some change here, but it will be slow.
Community Based Care – With more people coming back into the healthcare system with Health Reform, there will be a greater need for location based access to healthcare. This will involve clinics but will be much broader. Companies will need to look at how they embrace community resources like churches to engage the disengaged and poor who don’t trust the system and have limited access to the traditional channels.
At the conference last week, I was talking about the opportunity for retail pharmacy to play a broader role as the patient’s medical home. As part of that discussion, I tried to create a vision of a digitally connected location. Here’s my summary of that…
Imagine that the pill bottle you use is now a smart object (expanding on the RxVitality concept). It now knows when you are running low on pills. Since it’s connected to your WiFi signal and to your smart phone, as soon as you’re low, it does the following:
Send a new refill request to the pharmacy (or to your physician if you’re out of refills)
Puts a reminder in your phone for you to pick up the prescription (action item list, calendar) and updates that once it gets confirmation on time from the pharmacy
As you’re driving by the pharmacy, your smart phone reminds you to pick up the Rx as it knows where you are based on GPS.
When you enter the pharmacy, it has a system to capture information from your devices or phone about your sleeping habits, what you’ve been eating, and your exercise. All of this information is important for them to actively manage your health. Additionally, as you enter the pharmacy, they use a technology like FaceDeals to recognize you and do several things:
Alert the pharmacy that you’re in the store so they can pull your prescription
Pull up your CRM (customer relationship management) profile so they pharmacist and tech can great you by name and link back to other information (i.e., Hi George. Are you here to pick up your prescription? By the way, how did those crutches work out?)
Offer you a coupon on some new OTCs or medical supplies based on your chronic disease(s)
While you’re shopping (at a grocery or big box pharmacy), you’re linking your smart phone to the smart cart which is helping you navigate the store. As it confirms your identify via fingerprint or facial recognition, it opens up a link to your medical data. This allows the cart to help you navigate the store and scans everything you put into the cart to look for drug-food interactions (e.g., grapefruit juice). It also helps to steer you to better food options (eat this not that) based on your diagnoses (i.e., for a diabetic, I would suggest this other cereal). All of this is happening on your screen to protect your privacy.
By the time you get to the pharmacy, you stand in front of the register which has a scale embedded in the floor so they can instantly know your weight and compare that to your last measurement. Since they are now tied into your medical data, the Point of Sale technology also gets relevant alerts that they can talk with you about (e.g., Did you know that your health coverage has changed? Did you know that you have access to a health coach to discuss your condition?).
As you leave, all of the data they collected is integrated and pushed out to both your personal health record (PHR) along with the electronic medical record (EHR) that your physician uses. Any new risks identified are also shared with your caregiver or others in your social circle that you’ve identified and opted-in to receive information. This social connectivity helps to create the village necessary to drive change.
Scary or fascinating? I prefer to think about this as a fascinating way of leveraging technology and data to make my experience better and improve my outcomes, but I know not everyone will feel that way.
I was reading the mHealth Trends and Strategies 2013 by netcentric strategies, and I thought I would share a few things from the report. Of course, I like the acronym SMAC which I re-used in the title and in a recent presentation.
Mobile phone use for health information reached 75M in 2012.
Tablet activity for healthcare reached 29M in 2012.
50% of people will download mHealth applications (prediction).
“mHealth is not a separate industry, but rather it’s the future of a healthcare industry that’s evolving to care for patients differently, putting them first to deliver services better, faster, and less expensively.” quote from David Levy, MD, Global Healthcare Leader at PwC
Only 27% of MD actively encourage patients to manage their own health through mHealth applications. (problem)
13% of MDs actively discourage mHealth participation.
There is a whole section on remote patient monitoring with some good points about the system and the financial case. There is another section on preventative technology talking about adherence and compliance. It makes a key point which I believe is that technology will be welcomed by the 7M long-distance caregivers.
And, if you haven’t heard the term yet – BYOD. This stands for Bring Your Own Device which is about letting the user chose the device / interface that works for them but being flexible in terms of normalizing the data and using it within the workflow that you develop.
I’ve been a longtime user of Garmin for my running. They provide easy to use GPS watches that provide you with all the details and history you want. I also now have my FitBit as another tracking device when I run.
So, while several people encouraged me to try RunKeeper, I was hesitant. How many trackers for the same activity do I need? But, I started carrying my iPhone for music while I ran so I decided to give it a try.
I like it.
So, the question is why?
It talks to you. While looking at my Garmin is pretty easy, the RunKeeper app speaks into my headphones while I’m running to tell me when I’ve completed a half-mile, what my total time is, what my average mile pace is, and what my last split was. I can certainly calculate all that and see it on my Garmin, but this is very easy.
It gives you reinforcement and now some badges (through Foursquare which I don’t use). But, I do like the reinforcement – i.e., that was your longest run, that was your fastest run. Simple but positive.
It has a nice GUI (graphical user interface) or app. It tracks my data. It’s easy to read.
So, if you’re like I was, I’d recommend trying it.
As I talked about in my post about Walgreens and innovation, Walgreens has renamed their TakeCare Clinics to Healthcare Clinics at some locations. This is more than just a meaningless name change. This is the beginning of a business model change. This is the shift from acute care to ongoing chronic disease management. This is a big move that changes their place in the healthcare value chain.
It’s part of the overall strategy that has pulled them into the ACO space.
It will be interesting to see if CVS Caremark and their MinuteClinics follow them. CVS Caremark already announced a different strategy in terms of providing advocates. If I were them, I would jump fully into the remote monitoring / mHealth space and provide chronic disease management from a remote basis. I think this would be different and innovative.
I’m excited to be presenting in the Fall with Adam Fein and lots of other great speakers at the 2nd Bio/Pharma Retail Strategy Summit to be held September 18-19 in Philadelphia, PA.
I get to talk about one of my favorite topics which is how health reform is driving change in the industry and enabling new opportunities for the pharmacy / pharmacist.
You get to listen to me for 90-minutes so I’m hoping to find some great examples, data, and insights to get you thinking hard about your business and the white space here. I hope to see some of you there. If interested, I’m passing on a discount code they offered to me as faculty.
I was monitoring a pharma conference over in Europe this morning. I found a few of the dialogues really interesting. One of them was about a company creating all these websites to allow consumers to engage with them. There was then some debate.
It’s not about the channel it’s about the strategy #digpharm
On the on hand, I can agree that you can do some creative things with the channel, and therefore, I should be too down on someone who is very web centric. (i.e., focus on the strategy) On the other hand, digital is much bigger than web.
I’m sure there’s a lot of views here, but let me share mine in terms of what to consider from a digital strategy:
A website or series of sites along with a mobile web optimization for devices
Search engine optimization
Social (e.g., Facebook, Google+)
Communities
Video
Mobile apps
Device integration (e.g., BodyMedia)
Software integration (e.g., EMRs, PHRs)
Blogging
Twitter
Gamification
Telehealth
Remote monitoring
Big Data
Predictive algorithms
Location based services (e.g., FourSquare)
Use of SMS
While there are a lot of complicated images out there trying to show everything around digital strategy, I found this one pretty simple and concise.
Today, I’m giving my presentation at the PBMI conference in Las Vegas. This year, I choose to focus on the idea of shifting from fee-for-service to value-based contracting. People talk about this relative to ACOs (Accountable Care Organizations) and PCMHs (Patient Centered Medical Homes) from a provider perspective. There have been several groups such as the Center For Health Value Innovation and others thinking about this for year, but in general, this is mostly a concept. That being said, I think it’s time for the industry to grab the bull by the horns and force change.
If the PBM industry doesn’t disintermediate itself (to be extreme) then someone will come in and do it for them but per an older post, this ability to adapt is key for the industry. While the industry may feel “too big to fail”, I’m not sure I agree. If you listened the to the Walgreens / Boots investor call last week or saw some of things that captive PBMs and other data companies are trying to do, there are lots of bites at the apple. That being said, I’m not selling my PBM stocks yet.
So, today I’m giving the attached presentation to facilitate this discussion. I’ve also pre-scheduled some of my tweets to highlight key points (see summary below).
As I mentioned a few weeks ago (2/2/13), I wanted to test and see if healthcare companies would respond to consumers via Twitter. To test this, I posted a fairly general question or message on Twitter to see the response (see below). Of the 23 companies that I sent a message to, only 12 of them ever responded even after 6 of them received a 2nd message. Those results are shared below. What I also wanted to look at was the average time to respond along with which group was more likely to respond.
PBMs – All of the 3 PBMs that I reached out to responded. (This could be biased by my involvement in this space since two of them e-mailed me directly once I posted a comment.)
Pharmacies – Only 2 of the 4 retail pharmacies that I reached out to responded.
Disease Management Companies – Only 1 of the 3 that I reached out to responded. (I was surprised since Alere often thanks me for RT (re-tweeting) them, but didn’t respond to my inquiry.)
Managed Care – 5 of the 7 companies that I reached out to responded. (For Kaiser, they responded once I changed from @KPNewscenter to @KPThrive.)
Health Apps or Devices – Only 1 of the 5 companies that I reached out to responded. (This continues to surprise me. I’ve mentioned @FitBit on my blog and in Twitter numerous times without any response or comment.)
Pharmaceutical Manufacturers – Only 1 of the 3 companies that I reached out to responded. (This doesn’t surprise me since they are very careful about social media. @SanofiUS seems to be part of the team that has been pushing the envelope, and they were the ones to respond. I thought about Tweeting the brands thinking that those might be monitored more closely, but I didn’t.)
I will admit to being surprised. I’m sure all of these companies monitor social media so I’m not sure what leads to the lack of response. [I guess I could give them the out that I clearly indicated it was a test and provided a link to my blog so they could have chosen not to respond.]
Regardless, I learned several things:
Some companies have a different Twitter handle for managing customer service.
Some companies ask you to e-mail them and provide an e-mail.
Some companies tell you to DM (direct message) them to start a dialogue.
From a time perspective, I have to give kudos to the Prime Therapeutics team that responded in a record 2 minutes. Otherwise, here’s a breakout of the times by company with clusters in the first day and approximately 2 days later.
Company
Response Time (Hrs:Min)
Prime Therapeutics
0:02
Aetna
1:12
LoseIt
1:19
Healthways
2:07
Walmart
3:01
Express Scripts
8:35
Kaiser
29:22
BCBSIL
47:32
OptumRx
47:39
BCBSLA
48:18
Sanofi
53:30
I guess one could ask the question of whether to engage consumers via Twitter or simply use the channel more as a push messaging strategy. The reality is that consumers want to engage where they are, and there are a lot of people using Twitter. While it might not be the best way to have a personal discussion around PHI (Protected Health Information) given HIPAA, it certainly seems like a channel that you want to monitor and respond to. It gives you a way to route people to a particular phone number, e-mail, or support process.
As Dave Chase said in his Forbes article “Patient engagement is the blockbuster drug of the century”, this is critical for healthcare companies to figure out.
The CVS Caremark team told me that they actively monitor these channels and engage with people directly. I also talked with one of the people on the Express Scripts social monitoring team who told me that they primarily use social media to disseminate thought leadership and research, but that they actively try to engage with any member who has an actionable complaint. They want to be where the audience is and to quickly take the discussion offline.
If you want to see the questions I asked along with the responses, I’ve posted them below…
Dr. Kraft (@daniel_kraft) recently spoke at FutureMed and talked about the prescribing apps era. I’ve talked about this concept many times, and I agree that we are rapidly moving in that direction. And, there’s lots of buzz about whether apps will change behavior and how soon we’ll see “clinical trials” or published data to prove this.
1) Mobile Phones (quantified self) are becoming constant monitoring devices that create feedback loops which help individuals lead a healthy lifestyle. Examples include; monitoring glucose levels, blood pressure levels, stress levels, temperature, calories burned, heart rate, arrythmias. Gathering all this information can potentially help the patient make lifestyle changes to avoid a complication, decrease progression of a particular disease, and have quality information regarding his physical emotional state for their physician to tailor his treatment in a more efficient manner.
2) The App prescription ERA: Just as we prescribe medications prescribing apps to patients will be the future. The reason why this is important is that apps created for particular cases can help the patients understand their disease better and empower them to take better control.
3) Gamification: using games in order to change lifestyle, habits, have been mentioned before. A very interesting concept was that created in the Hope Labs of Stanford. The labs created a game in which children would receive points after there therapeutic regiment, once points were optioned they could shoot and attack the tumor. Helping with the compliance rate of the treatments
4) Lab on a chip and point of care testing
5) Artificial Intelligence like Watson and its application in medicine.
6) Procedure Simulation: Several procedures done by medical professionals follow (not 100%) a see one, do one teach one scenario. Probably very few people agree with this concept and that is why simulation has great potential. In this case residents, fellows in training can see one, simulate many and then when comfortable do one.
7) Social Networks and Augmented Reality
At the same time, a recent ePocrates study hammered home the point that while this is taking off physicians don’t have a mechanism for which ones to recommend and why.
According to the Epocrates survey, more than 40 percent of physicians are recommending apps to their patients. In terms of the apps being recommended, 72 percent are for patient education, 57 percent are lifestyle change tools, 37 percent are for drug information, 37 percent are for chronic disease management, 24 percent are for medical adherence and 11 percent are to connect the patient to an electronic health record portal.
Physicians also have several different sources for identifying which apps to recommend to their patients. According to the survey, 41 percent get advice from a friend or colleague, while 38 percent use an app store, another 38 percent use an Internet search engine, 23 percent learn of an app from another patient or patients, and 21 percent use the app themselves.
That said, the survey also notes that more than half of the physicians contacted said they don’t know which apps are “good to share.”
As I’ve discussed before, this is somewhat of the Wild West. Patients are buying and downloading apps based on what they learn about. They’d love for physicians, nurses, pharmacists, and other trusted sources to help them. But, those clinicians are often not technology savvy (or at least many of the ones who are actively practicing). There are exceptions to the norm and those are the ones in the news and speaking at conferences.
IMHO…consumers want to know the following:
Which apps make sense for me based on my condition?
Will that app be relevant as I move from newly diagnosed to maintenance?
Should I pay for an app or stick with the free version?
Is my data secure?
Will this app allow me to share data with my caregiver or case manager?
Will this app have an open API for integration with my other apps or devices?
Is it intuitive to use?
Will this company be around or will I be able to port my data to another app if the company goes away?
Is the information clinically sound?
Is the content consumer friendly?
Is it easy to use?
Is there an escalation path if I need help with clinical information?
Will my employer or health plan pay for it for me?
Is my data secure?
And, employers and payers also have lots of questions (on top of many of the ones above):
Is this tool effective in changing behavior?
Should I promote any apps to my members?
Should I pay for the apps?
How should I integrate them into my care system?
Do my staff need to have them, use them, and be able to discuss them with the patient? (Do they do that today with their member portal?)
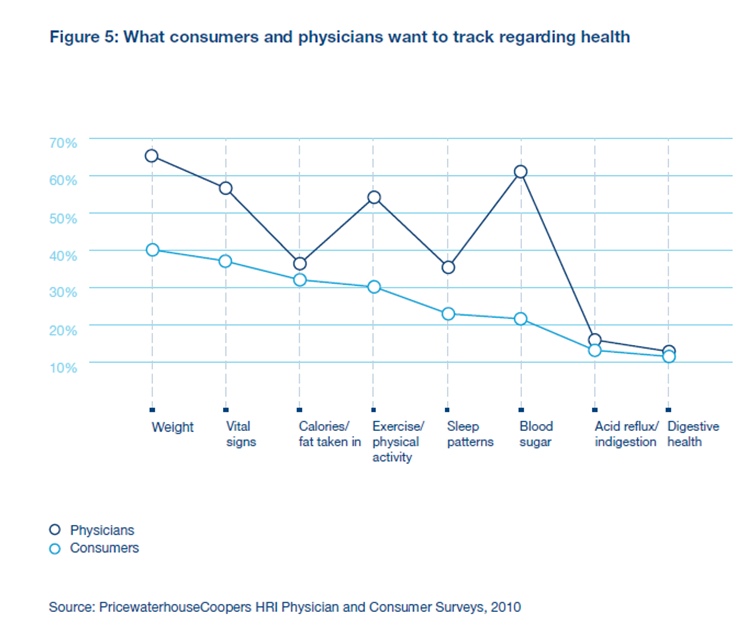
With all the discussions these days on Big Data and how to use information to create insights and wisdom, I was really shocked when I looked back at this PWC survey from 2011. In it, less than 1/3rd of health insurers were very confident in their use of informatics to add value around case management, disease management, wellness, and consumer health tools. WHAT???
This seems crazy to me. In this interconnected world where everyone is talking about connected devices, mHealth, and ENGAGEMENT, health insurers are in the optimal position to leverage their data to provide insights, to provide transparency, to create algorithms, to be preventative in their actions, etc. Maybe their technology platforms are too old? Maybe they’re too silo’d? I’m not sure. But, I find this an interesting arbitrage opportunity.
With a system that integrates data from claims, labs, patient reported sources, HRAs, and biometrics, you can add value by creating a personalized patient experience that adapts with their needs.
In the Winter 2012 Innovate Magazine from Barnes-Jewish Hospital and Washington University Physicians, they talk about a new iPad app that they developed that calculates disease risk and offers a customized plan.
I just downloaded it and used it. Here’s my quick summary:
Nice GUI (graphical user interface)
Easy to use HRA (health risk assessment)
Cool interactive tool (you can see how your risk for certain diseases changes with your changes in behavior)
Content seems to be well written with basic health literacy taken into account
Links out to more research and content
Messaging feature (which I guess will push me updates and other messages over time)
Overall, it seems like a nicer than normal HRA with the ability to interact with it. My question would be how it integrates with my care team and how it gets used over time. If this integrated into my other devices and monitored my data, it would seem more valuable than a standalone app, but I certainly think it’s great for a one-time use.
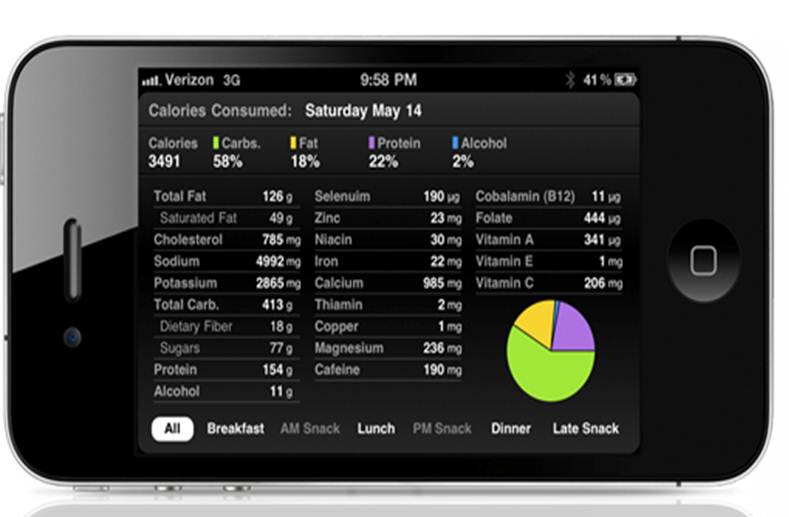
In the spirit of the Quantified Self movement and in order to better understand how mHealth tools like FitBit can drive behavior change, I’ve been using a FitBit One for about 6 weeks now. I’ve posted some notes along the way, but I thought I’d do a wrap up post here. Here’s the old posts.
The user interface is simple to use. (see a few screenshots below)
I feel like it works in terms of helping me learn about my food habits. (Which I guess shouldn’t be surprising since research shows that having a food diary works and another recent study showed that a tool worked better than a paper diary.) For example, I learned several things:
I drink way too little water.
I eat almost 65% of my calories by the end of lunch.
Some foods that I thought were okay have too many calories.
In general, the tracking for my steps makes me motivated to try to walk further on days that I’m not doing good.
The ease of use and simple device has helped me change behavior. For example, when I went to go to dinner tonight, I quickly looked up my total calories and saw that I had 600 calories left. Here’s what I ate for dinner. (It works!)
But, on the flipside, I think there are some simple improvement options:
I eat a fairly similar breakfast everyday which is either cereal with 2% milk and orange juice or chocolate milk (if after a workout). [In case you don’t know, chocolate milk is great for your recovery.] Rather than have to enter each item, FitBit could analyze your behavior and recommend a “breakfast bundle”. (and yes, I know I could create it myself)
Some days, I don’t enter everything I eat. When I get my end of week report, it shows me all the calories burned versus the calories taken in. That shows a huge deficit which isn’t true. I think they should do two things:
Add some type of daily validation when you fall below some typical caloric intake. (Did you enter all your food yesterday, it seemed low?)
Then create some average daily intake to allow you to have a semi-relevant weekly summary.
The same can be true for days that you forget to carry your device or even allowing for notes on days (i.e., was sick in bed). This would provide a more accurate long-term record for analysis.
The food search engine seems to offer some improvement opportunities. For example, one day I ate a Dunkin Donuts donut, but it had most types but not the one I ate. I don’t understand that since there’s only about 15 donuts. But, perhaps it’s a search engine or Natural Language Processing (NLP) issue. (I guess it could be user error, but in this case, I don’t think so.)
Finally, as I think about mHealth in general, I think it would be really important to see how these devices and this data is integrated with a care management system. I should be able to “opt-in” my case manager to get these reports and/or the data.
The other opportunity that I think exists is better promotion of some things you don’t learn without searching the FitBit site:
They’re connected with lots of other apps. Which ones should I use? Can’t it see which other ones I have on my phone and point this out? How would they help me?
There’s a premium version with interesting analysis. Why don’t they push these to me?
And, with the discussions around whether physicians will “prescribe” apps, it’s going to be important for them to be part of these discussions although this survey from Philips showed that patients continue to increasingly rely on these apps and Dr. Google.
Finally, before I close, all of this makes me think about an interesting dialogue recently on Twitter about Quantified Self.
Last week at the mHealth Summit in DC, I had a chance to sit down and visit with Christine Robins who is the CEO of BodyMedia. (see bio below) One of the most exciting things (mentioned at the end) is their new disposable solution coming out.
Christine Robins is currently the Chief Executive Officer of BodyMedia, Inc., a pioneering market leader in wearable body monitors. BodyMedia’s devices are unparalleled in the marketplace, and equip professionals and consumers with rich information to manage a range of health conditions impacted by lifestyle choices.
Prior to joining BodyMedia, Christine was the CEO of Philips Oral Healthcare where she led the global Sonicare® brand to significant sales and share growth. Christine also has extensive experience in a wide range of marketing and finance capacities gained during her 17 years at S.C. Johnson, where she ran notable brands such as Raid® insecticides, Glade® air fresheners, and Aveeno® skin care. With this background rooted in global multi-national companies and an entrepreneurial zeal essential to lead a high technology upstart, Chris is passionate about developing turnaround strategies, building teams, and driving innovation.
A noted speaker, Christine has delivered presentations at universities such as Harvard, Stanford and Duke, as well as keynotes at industry shows such as the Consumer Electronics Show, Health 2.0 and CTIA. She holds a degree in Marketing and Finance from the University of Wisconsin-Madison and an MBA from Marquette University.
If you’re not familiar with BodyMedia, it’s definitely a company to know from a Quantified Self perspective. They have been around since 1999 providing solutions and have 150 global studies about the effectiveness of their devices in weight loss (see one chart below). The devices that they use continue to get smaller and smaller with time and are registered with the FDA as Class II medical devices.
Their devices track 5,000 data points per minute using 4 different sensors. Here are a few screen shots from the mobile apps that they have.
And, as you can see, they map well to the chart below which shows what data consumers and physicians want to track with weight, calories, physical activity, and sleep patterns.
For food tracking, they work with MyFitnessPal which provides them with data on products you eat. I think a good example can be seen in this screen shot from the Android app.
But, honestly, a lot of what I was really intrigued by was a new offering they’re rolling out called the “PATCH” which will be a 7-day, disposable body monitoring system that does everything the full blown system does. I don’t know the price point yet, but this is really exciting as a way to pull new people into the market and to use as a strategy for setting a baseline with a patient to understand their data. It could then lead to recommendations around disease management.
Another thing that Christine talked about was they’re approach to partnering with places like the Biggest Loser and other to allow for a customized content approach to your messaging from the system. She also showed me how the device will project where you will end up at the end of the day based on your past history.
They also have a module for a coach or weight loss professional to help manage and view data across all the people they’re working with.
(And, I just grabbed this image from their website since it points out the 3 key things to weight loss.)
I only had time to attend one day of the mHealth Summit in DC. Overall, it seemed like a well attended event with a good vendor area.
But, what I saw left me with concerns about the maturity of the space.
1. Every vendor has their own portal. There was no idea of convergence or sensitivity to the care manager or provider or patient having to access multiple sites to collect data. Of course, there were a few exceptions.
2. There’s still some heavy lifting for the consumer, but it’s getting better. For example, one food application lets you scan in your food but that calorie counter isn’t integrated into any activity monitor. Another application was trying to monitor social activity for part of their depression algorithm but they weren’t leveraging the data sitting on the phone itself – numbers of calls, movement, etc.
3. There are some really creative solutions being tried but the scale of the studies is small. I was excited to see what was being done with obesity, but the case studies were less than 150 participants.
4. There are a lot of non-healthcare people jumping in which is great from an innovation perspective, but healthcare is tricky and making sure to apply consumer literacy filters to the clinical guidance you get is important. For example, I asked one vendor why he had several chronic diseases covered but ignored high cholesterol. He pointed out that he had a heart disease component, but IMHO I don’t know many people with high cholesterol that would self select into heart disease.
On the other hand, there were some really positive things.
1. The user interface on a lot of these is very elegant.
2. The devices are getting smaller and smaller with a few disposables on the way.
3. The data captured and reporting is really interesting and insightful although I’m not sure how it will all be used by patients, physicians, or companies.
4. Technology is much more scalable than people centric strategies which is critical in the US and globally.
5. Several companies really get it and are focused on device neutral approaches for capturing and disseminating data.
Overall, it reminded me of some of my concerns about the Health 2.0 movement a few years ago in terms of business models and distribution models. But, keep the innovation coming. It’s fascinating and thought provoking. But, there will definitely be a shakeout in the years to come.
It’s always fun to predict what will happen in the next year. No one is ever right, but you can hope to be directionally correct. With that in mind, here’s a few of my thoughts for what will happen in 2013…
Reform (PPACA aka ObamaCare) will happen. While the Republicans will fight it, with Obama’s re-election and the Supreme Court decision. Reform will continue to happen. The states will mess up the Exchanges which will create many issues, but private exchanges will come to the “rescue”.
“Big Data” will be a focus at every healthcare company. What data to store? How to mine the data? What data to integrate? How to bring in unstructured data such as physician’s notes? What to do with consumer reported and consumer tracked data from all the different devices?
Physicians will emerge back in the power seat. With Accountable Care Organizations and Patient Centered Medical Homes, consumers are finally becoming more aware of all the shortcomings in our sick care system. They trust their physicians although somewhat blindly given ongoing challenges with evidence-based care and quality which are often the result of our Fee For Service system (too little time) combined with an abundance of new research happening concurrently.
mHealth will be the buzz word and exciting space as entrepreneurs from outside healthcare and people with personal healthcare experiences will attempt to capitalize on the technology gap and chaos within the health system. This will create lots of innovation, but adoption will lag as consumers struggle with 15,000+ apps and the sickest patients (often older patients) are the slowest to adopt.
Device proliferation will go hand in hand with mHealth and with the Quantified Self movement. This will create general health devices, fitness devices, diabetes solutions, hypertension solutions, and many other devices for wellness and home monitoring for elderly patients. Like mHealth, this will foster lots of innovation but be overwhelming for consumers and lead to opportunities for device agnostic solutions for capturing data and integrating that data for payors and providers to use.
The focus on incentives will shift in two ways. Technology vendors will begin to look more and more at the gamification of healthcare and how to use gaming theory and technology to drive initial and sustained engagement. At the same time, the recent ruling will allow employers to shift from rewards to “penalties” in the form of premium differentials where patients who don’t do certain things such as take biometric screenings or engage with a case manager will pay more. In 2014 and 2015, this shift will be from penalties with activity to penalties tied to outcomes.
Consumer based testing will drive greater regulation. With the focus on home based testing (e.g., HIV or High Cholesterol) and the increased interest in genetic testing especially when tied to a medication, the FDA and other government agencies will have to address this market with new regulations to close gaps such as life insurance companies being able to force disclosure of genetic testing in order to get coverage (even though the testing isn’t necessarily deterministic).
Clinics will prepare for 2014. With the increase number of consumers being covered in 2014, there will be an access challenge for patients to see a provider. This will drive buildout and utilization of health clinics such as TakeCare or MinuteClinic. Clinics will have to look at how to adapt their workflow to create a patient relationship which will create potential integration points with TeleHealth and bring back up the issue of whether they should or could replace the traditional Primary Care Provider (PCP) relationship or not.
Telemedicine will hit a tipping point and begin to Cross the Chasm. They now have better technology and adoption within major employers. This will start to create more and more business cases and social awareness of the solution. With utilization, we will see great adoption and the increasing use of smart phones for healthcare will drive telemedicine into an accelerated growth stage.
Transparency solutions will continue to be a hot area with CastLight and Change Healthcare leading the way. Their independence and consumer engagement approaches based on critical moments (i.e., pointing out how to save money on Rxs just before a refill) and using multiple channels will show high ROI which will also increase broader healthcare awareness making them part of the population health solution.
Generics will no longer be a talked about issue. With generic fill rates running so high across different groups and being front page news, PBMs, pharmacies, and pharma will truly begin to move forward to embrace the specialty market with a clear vengeance (at least in the US).
There are still a few longer term trends that I’m watching, but I don’t think that 2013 is the primary year for them.
The evolving role of pharmacists within the Medical Home and with vaccines.
A significant shift from mail order to 90-day at retail fulfilled by massive central fill facilities.
Pharma co-opetition where they begin to collaborate at the disease state level realizing the a rising tide is good for all boats.
Integration of data from all types of solutions and actions into workflow triggers that automatically create new events within the care management infrastructure using Service Oriented Architecture and Business Process Management.
I’ve shared a few tests with you about my FitBit One which included comparisons against my Garmin and versus a pedometer. Today, I got to take it to the gym with me and tested it for distance and calorie count relative to several pieces of equipment from LifeFitness – treadmill, stationary bike, and elliptical. For the treadmill, I also looked it two ways: (1) running at an 8 minute mile pace and (2) walking at a 15 minute mile pace at a 15% slope.
As you can see before, the FitBit was much better aligned on distance with the treadmill, but it was not as aligned on calorie count. I’m have no hypothesis here. I will say that I was surprised that the uphill walking didn’t somehow register as steps. I say that because I went on an outside run the other day up and down hills, and the FitBit did a great job of tracking my uphill runs and translating that into floors climbed.
As a side note, I think this does a nice job (if you believe the equipment calorie count) on showing how a slow walk up a steep slope can burn lots of calories compared to a fast run.
NOTE: The opinions expressed here are those of the author and are not reviewed in advance by anyone but the individual author. They represent personal opinions not the opinions of any employer.

 June 2, 2014
June 2, 2014