
 October 23, 2012
October 23, 2012 
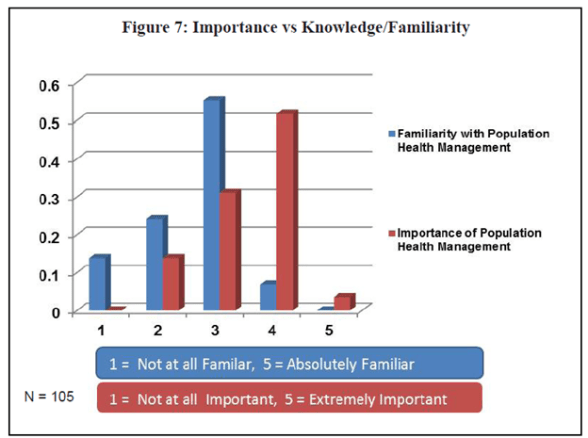
The ideas around Population Health are certainly critical both to us as a country to eliminate the waste in our healthcare system, but they are also foundational in a move from a fee-for-service (FFS) environment to an outcomes-based payment model. Interesting, if you look at a study that was just released, it continues to show a disconnect within the provider community. (Study is Population Health Management In Physician Practice: A Call To Action.)
I believe some of this stems from the costs associated with the build out, integration, and use of these technologies in today’s environment. But, I think some of this stems from a broken connection between national policy, localized implementation, and payer coordination around key healthcare issues such as obesity.
The following paragraph from the same document is also very telling.
“With 72% of respondents reporting that they had either already adopted or were in the process of adoption a patient-centered model of care, it was interesting that only 19% of practices self-reported as Patient-Centered Medical Home (PCMH) and only 10% as an Accountable Care Organization (ACO). Considering the critical role that population health management will play in both types of practice models, the data suggest that while they are undertaking population health management initiatives, many practices may not yet be at a level of transformation to warrant presenting as PCMH or ACO at this point in time. Also interesting is that of the 11 practices that did self-report as ACO, only 5 of the 11 also reported as PCMH – showing again perhaps another disconnect or struggle with implementation and understanding. PCMH, after all, has been described as “foundational” to Accountable Care Organizations.”
A lot of this change won’t be done by physicians, but it was promising to hear in the same report that:
- 96% of large provider practices employed Nurse Practitioners;
- 70% employed Physician Assistants; and
- 91% employed Care Coordinators.
So, how are those resources being used today? And, how do these resources get integrated into an overall care strategy for the patient? Are notes shared with external care managers? How do we find the right point person? How does an external payer team for MM coordinator with the local resources for something like discharge planning?




No comments yet... Be the first to leave a reply!