
 December 16, 2010
December 16, 2010 
Milliman recently put out a whitepaper commissioned by ReStat on “Alternative Pharmacy Network” savings. My general opinion is that they use a lot of data and analysis mixed with some sensationalist statements to make the very obvious point that creating a limited or closed pharmacy network will save you money. (I hope they didn’t charge much for this.)
Net-Net: Limited or tier pharmacy networks are a great idea. ReStat is building on their experience with Caterpillar which is a great program. But, the whitepaper was flawed.
Their conclusions were:
- Potential Savings – The analysis shown in this report suggests that APN programs can offer a significant savings to employers relative to traditional networks. For an assumed range of consumer use of participating pharmacies, an employer with 10,000 lives could save $200,000 to $620,000 per year, depending on benefit design, without changing cost-sharing structures (see Table 3). Benefit design changes could increase or decrease the savings. A closed APN network (no coverage for non-APN pharmacies) would increase savings for a given benefit design.
- Sources of Savings – In our analysis, the APN model can achieve lower cost because the PBM and retail pharmacy retain less revenue.
- The Value of Limited Networks for Pharmacies -For medical benefits, health plans use network providers as part of overall quality and efficiency programs and are promoting network programs such as medical homes and pay-for-performance. Sponsors and PBMs can extend the advantages of networks to the pharmacy benefit. However, the ability to obtain value in a locale depends on the willingness of some pharmacies to participate as network members.
- Plan Design Changes – Plan sponsors may need to change their plan designs to encourage use of the limited network. For example, the copays for limited network pharmacies may need to be decreased (from current levels) and/or the copays for non-network pharmacies may need to be increased to create a benefit differential between the network and non-network pharmacies. These plan design changes could reduce or increase the projected savings of a limited network, depending on the specific change.
My comments about their analysis:
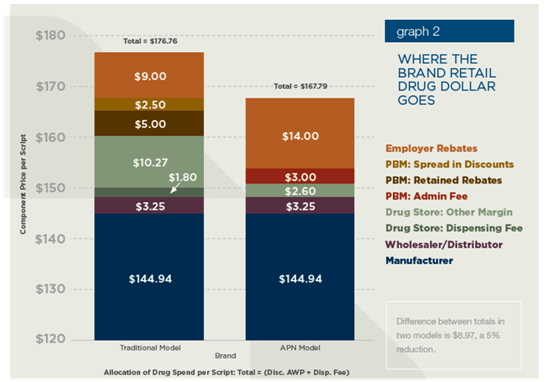
- They assumed that retail pharmacies would reduce their spread on generics by 44% (and brands by 78%) to be part of a limited network. That might be true for a large client with geographic concentration and for a retailer with low market share, but I think that’s a leap. (see chart below on brand pricing assumptions)
- They say that spread for retail claims for PBMs can be 10-15% of AWP. I’ve seen plenty of deals that were negative (at least on brand drugs). In many cases, spread pricing doesn’t even exist.
- They claim that PBM’s make money “(as part of a typically Drug Utilization Review program) actively encourages patients to switch to different medications as a core part of its business.” Really. That went out with the AG settlements back around 2004. Chemical substitution to generic equivalents certainly happens, but using DUR to push therapeutic conversion. I don’t think so.
- They claim that PBM’s will buy drugs and repackage them to get a higher reimbursement rate at mail. I’ve never seen it (but that doesn’t mean it’s not done).
- MAC pricing at mail. Yes. PBMs do make most of their money on generics at mail, and I’ve talked about the need to align your MAC lists at retail and mail before.
- They also say “While mail order presents the opportunity to save sponsors money, attempts to encourage mail order by reducing copays could increase sponsor cost if the benefit plan is poorly designed (e.g., copays are reduced too much), utilization increases, or generic dispensing decreases.” I’ve talked about why clients lose money at mail before, but I’m pretty sure that there have been plenty of studies that show adherence improves (not unnecessary utilization). Studies have also shown that if you adjust for acute medications at retail then the generic dispensing rates are very comparable at retail and mail (or explained thru population differences).
- They claim that the PBM’s make 10-15% on specialty drugs that they dispense (which seems high to me) and then use $5,000 per month as a number when the average 30-day supply of a specialty drug is more like $1,500.
- They claim “Different manufacturers offer different rebates, which may factor into a PBMs decision making.” I think if you read the P&T process documents you would see that decisions about in or out are made based on clinical decisions and then a formulary can be broad or narrow based on the net price to the plan sponsor which does (and should) evaluate rebate impact.
- They quote a source saying that 35% of rebates are kept by PBMs. Again, that seems really high. In my experience, there was an administrative fee equal to several percent of the AWP of the drug that was kept but the rebate dollars were passed to the plan sponsor.
While I like the simplicity of the flat fee payment model (i.e., I pay my PBM $3.00 per claim), it certainly creates no incentive for them to do better year over year in improving their negotiating with pharma and retailers or to worry much about trend management.
They talk briefly and seem to encourage ReStat’s Align product which seems like a very logical approach (used by other PBMs also).
Restat configures custom retail networks and benefit designs that create incentives to encourage member use of alternative in-network pharmacies and allows consumers the ability to shop based on price as well as service. Non-network pharmacies are also available but at a higher copay or costs.




Since several people misinterpreted my post, I added the quote at the top today. The point of this was not a focus on ReStat or Align. They are built upon the Caterpillar model which has been one of the more revolutionary models over the past few years. I just didn’t like the data that Miliman used or the fact that they tried to throw the PBM under the business using old examples.
You can have a good successful PBM model and support a limited or tiered network.
I agree that the Milliman paper uses a lot of words to reach an obvious conclusion, but I feel the underlying reason for the papers efforts was to further encourage the use of PBMs. The paper uses a highly inflated profit margin of the existing PBM model, reduces those margins only slightly, leaving plenty of room for excessive profits during the Restat adjudication process.
Regarding your bullets points:
Number 3) Repackaging does occur and occurs frequently, allowing a new NDC to be assigned to the product and often a new AWP.
Number 7) Though the P&T process “in or out” is clinical in nature the tiering and/or copay process once on the formulary is not clinical but rebate driven
Number 8) 35% rebate retention is low not high. As a small PBM we once used a large PBM as a rebate manager. In law suit brought within the last 5 years we forced this PBM to divulge rebate information to all their clients using them as a rebate manager. We receive this report today on quarterly basis and the rebate retention still exceeds 90%.
I do agree that a limited access network design is the road to take. However, the access should be based on quality and total health care cost reduction, a “Centers of Excellence” (COE) network. A network of drug distribution that states it will make prescriptions passing through their portals perform to make the clients healthy and more productive workers.
Not Access, Not price, but performance: performance that yields healthy employees is the only way to lower health cost both drug and medical.
I also believe that the community pharmacist is the route to take to achieve this overall reduction in health care cost.
Jim Fields RPh CFO ApproRx