October 30, 2008
October 30, 2008 
If interested, I am going to host a webinar for managed care companies and PBMs. (Sorry, but this is limited to clients and prospects only.)
Proactive Cost Savings Programs for Your Members
In these economic times, members are looking for all the opportunities they can find to save money and reduce their out-of-pocket spending. This is a great time to drive loyalty by proactively interacting with your members and helping them understand how to save money.
Some of the timely communication programs that will make an impact include:
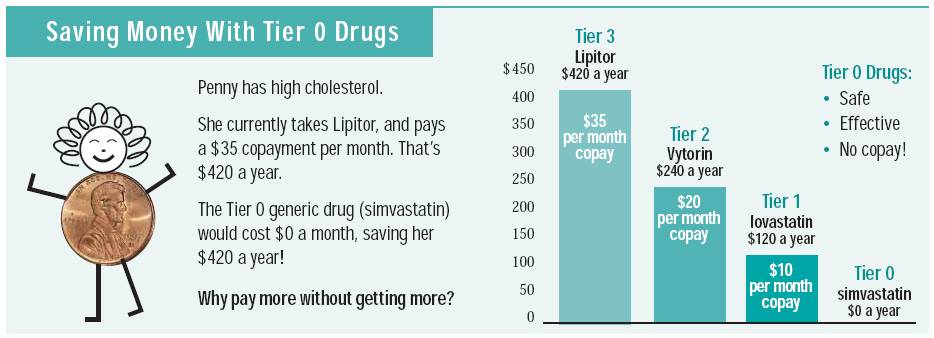
- Movement to generics (i.e., therapeutic interchange)
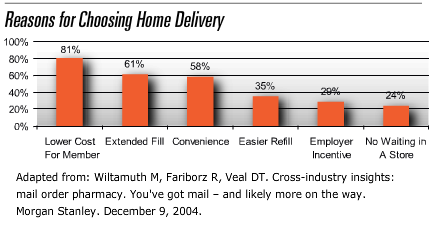
- Movement to mail or 90-day retail
- Pill splitting or dose consolidation
This is true for your commercial members as well as your Medicare members who are in the “donut hole”. Don’t let your members struggle and end up skipping doses or not taking their medication. This can lead to much bigger issues downstream.
Join Silverlink Communications for this interactive webinar and learn how you can design communication programs that help your members save money while improving your bottom line.