
 March 10, 2008
March 10, 2008 
Frederick Navarro is a research psychologist who, over the past 20 years, has focused his efforts on understanding people and the factors that shape their attention to health and care seeking. He has developed a unique model that approaches health care consumer behavior from a different angle than other models today. Over the past 10 years he has done considerable work with health plans and his findings often fly in the face of conventional thinking. He posted a long comment on my post the other day about Price and Placebo effect that I thought I would post here as a “guest post”.
On the issue of predictable irrationality and perception, what about the situation where a group of people rate their health status much better than another group of people, but the first group generates nearly twice the level of medical claims as the poorer health status group. That’s counter to the current belief that health status drives claims. So, what’s going on?
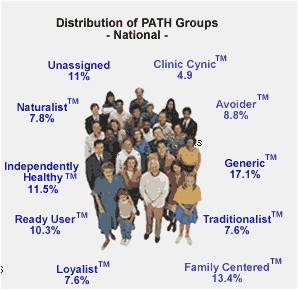
[His methodology divides people into PATH ( Profiles of Activities and Attitudes Toward Healthcare) Groups as shown below.]
Well, the difference is how each group of people judge when it is time to seek care. When do they say, it is time to go to the doctor? Type 2 people only go to the doctor when problems are serious. They ignore their health and are apathetic towards it. They have health problems, but they just live with them. Type 7 people go to the doctor at the first sign of a problem. They monitor their health and are very proactive about it. If something appears, they seek care for it. These are the types of people it seems the health industry wants to build more of to reduce costs.
In a 1995 study of Kaiser members in Hawaii, the Type 2 members rated their health status 11.9 (SF-12 scale) and Type 7 members rated their health status at 14.3. The Type 2 group had avg claims pmpy of $1,541; the Type 2 group had avg claims pmpy of $2,040. Whoops! The higher health status Type 7’s had nearly twice the claims as the lower health status Type 2.
Let’s bring things closer to present time. In 2004/2005 year long study of Cigna members in a DM program the same patterns were there. At the baseline, the Type 2 group reported avg health status of 3.26 (1 to 5 scale) and the Type 7 group reported avg health status of 3.45. Type 7 were higher again! Type 2 avg claims pmpy were $6,176. Type 7 avg claims pmpy were $9,910. Whoops again! After a year, the DM intervention did not change this. At the end of the study, Type 2 people reported health status at 3.3 (a touch better), and the Type 7 people reported health status at 3.54 (a touch better again). The Type 2 group’s claims went down to $4,750 pmpy. That’s over a $1,400 drop. The Type 7 groups claims after 1 year of DM intervention dropped to $9,017 pmpy (almost a $800 drop). The Type 7 higher health status group still had claims that were nearly twice the level of Type 2.
The moral to this story is that the predisposition to seek care is a huge driver of health care costs. In some groups of people it overrides their perception of their health. In the 1995 study and the 2004/2005 study, the reason why the Type 7 people had higher claims is because they came in demanding care. That’s all. And the doctors are happy to see them!
This all harkens back to an earlier blog where you discussed the Dutch study and how preventive care did not lower health care costs. Providers have convinced everybody that the cure to lower health care costs is to encourage more people to become like Type 7 and to make care more accessible and affordable.
Predictable irrationality?
Looks like it to me.






No comments yet... Be the first to leave a reply!