As if it’s not already difficult for patients to navigate their benefits, DTC advertising, and all the healthcare information on the web, it seems we are structurally trying to make it more difficult. With the recent news around Vytorin and Zetia, the drugs used to treat high cholesterol have gone through some dramatic changes over the past few years. (Here is the formal study.)
In an editorial by the New England Journal of Medicine:
“Until such data are available, it seems prudent to encourage
patients whose LDL cholesterol levels remain elevated despite
treatment with an optimal dose of a statin to redouble their
efforts at dietary control and regular exercise. Niacin, fibrates,
and resins should be considered when diet, exercise, and a statin
have failed to achieve the target, with ezetimibe [Vytorin] reserved for
patients who cannot tolerate these agents.”
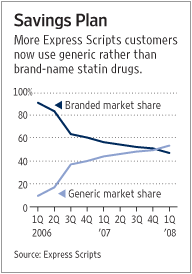
For several years, Lipitor was clearly the market leader with Zocor as a close second. Even with one drug (Mevacor) available generically, most plans (other than Kaiser) had single digit utilization. Kaiser was able to drive significant use of generic Mevacor as a first-line agent. When Zocor was going to lose it’s patent protection in 2006, most plans began moving Lipitor to the 3rd tier and introducing programs to move Lipitor patients to Zocor (generic name simvastatin). These included step therapy programs along with simple copay incentives by having a large copay differential between the 1st or 2nd tier and the 3rd tier.
Then, last year, Pfizer, which makes Lipitor, began to offer aggressive discounting to encourage some plans to actually encourage Lipitor utilization over generic Zocor. All the while, Vytorin and Zetia were gaining marketshare to capture a $5B piece of the market. Now, with the recent study, the authors are suggesting that these patients should be on generic Zocor or another drug in the statin class. I am sure there are some clinical nuances here, but the quote above seems to limit them.
And, of course, patients should discuss this with their physicians. They shouldn’t stop taking their drugs. And, generally, when you switch drugs, you want to get lab work done in this class. So, are we asking patients to change drugs again? Do they incur an office visit copay? Do they need to pay for the lab test?
Talk about confusing. And, at the same time, the Improve-It study around Vytorin and Zetia is enrolling more patients. Seems counterintuitive to the data just released.
I’m not a pharmacist, but after working in the industry, if I can’t figure out what to do, how can your average patient. At this rate, healthcare will be as confusing as our taxes.
Note: There are a handful of entries on this out at the WSJ Health Blog.

 April 18, 2008
April 18, 2008 






 Someone asked me if I thought pharmacists would be allowed to prescribe medication to patients. I’m not familiar with any legislation on this topic (although there well might be some).
Someone asked me if I thought pharmacists would be allowed to prescribe medication to patients. I’m not familiar with any legislation on this topic (although there well might be some).