September 3, 2008
September 3, 2008 
“Healthcare payer spending on business intelligence, information delivery and transparency is the fastest growing spending category in 2008 for healthcare payers,” said Janice Young, IDC Program Director, Payer IT Strategies.
This quote was in our press release this morning around the growth at Silverlink. You can read about the company in the release, but I wanted to focus on this quote from IDC.
On the one hand, I think consumers should be saying “Amen!” that payers are focusing on business intelligence (BI) although that can mean a lot of things. On the other hand, they would shocked to know how new this is to the healthcare space compared with the consumer packaged goods industry. BI can help identify gaps in care and identify how to help patients become better. BI can help personalize the messaging that you receive from your health plan so you don’t have these huge legal caveats about all savings and other specifics being based on your exact plan design and deductible.
Information delivery can also mean a lot of things. Is this reporting to the employer? Is this online analysis for the consumer? Is this communications?
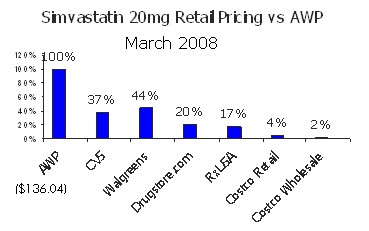
And, I am not sure what transparency means, but I hope it means things like letting consumers actually understand the price of goods and services and how to make tradeoffs between different options with all the data (e.g., quality, price, outcomes, patient experience).
Overall, for those of us in the healthcare communications space, this is a rising tide that helps. It means the payers who support all of you consumers are raising the bar and looking at how to use their information to improve the experience and outcomes (ideally). It could also allow them to better focus their efforts on the riskiest patients and discover the best way to drive behavior.
The data is there and has been there so figuring out how to use it and what to use it for is critical. Mapping this against the patient expectations and desired activities can be a great positive for the consumerism movement. Integrated data. Accessible data. Digestible data. Sounds great.