
While I’ve moved most of the infographics I find to my Pinterest account, I wanted to capture and share this one from Stephen Wilkin’s blog since it hits so many of the points that I try to make with people.

 June 11, 2013
June 11, 2013  2 Comments
2 Comments
While I’ve moved most of the infographics I find to my Pinterest account, I wanted to capture and share this one from Stephen Wilkin’s blog since it hits so many of the points that I try to make with people.
June 11, 2013 0 Comments
When I worked as an IT consultant, you had two clear choices – an enterprise system (e.g., SAP) or a best-of-breed (BOB) strategy. People liked the simplicity of an enterprise system, but you may have sub-optimized reporting or some flexibility in your solution. On the other hand, the BOB strategy required more maintenance, effort, and coordination to pull it off in a coordinated fashion.
In today’s healthcare world, I look at and meet with a ton of technology companies. The struggle is how to keep up with all the change in the industry and be nimble enough to engage the new start-up, but flexible enough to evolve with the market without impacting the consumer experience.
Maybe it draws on my training as an architect, but I was describing my technology vision as one of a general contractor. The buyer (client) wants a BOB solution. They want everything optimized – data, reporting, workflow, content, mobile, clinical algorithms, etc. At the same time, they often underestimate what it takes to manage all of these vendors, integrate the data on the backend, and create an integrated consumer experience across multiple vendors and technology platforms.
That’s where I see some real value add as a “technology curator”. I see one of my roles in helping manage an evolving ecosystem of healthcare companies and working with a flexible technology platform that can quickly plug and play with different solutions. This also allows me to have pre-built integrations with certain solutions, but I can also offer consumers the ability to choose their device (for example) and with the right API set up just be device agnostic in my solution.
Over time, this offers clients a lot of flexibility. The get the BOB approach within an enterprise system environment. They don’t have to keep issuing RFPs and evaluating vendors (since we’re doing that). They don’t have to stitch together multiple data sets to create the integrated, longitudinal view of the consumer (since we’re doing that). They don’t have to pretend that they’re offering a cohesive consumer experience (since we’re doing that). And, most importantly, they are flexible over time to jump from solution to solution within the architecture without disrupting everyone since it’s behind the “presentation layer” that the consumer experiences.
June 7, 2013 0 Comments
I saw this quote of the day in Drug Benefit News, and it made me think about all the discussions I’ve been having around population health management and the need for a longitudinal patient record and integrated member experience.
Medication therapy management (MTM) at its core is viewing “the member in its entirety and not as individual activities…and looking at all of those things around medications for that patient. You can have the best programs in the world but if the patient is not engaged, they are a waste of time and energy, and that’s why an integrated activity like MTM has the opportunity to be so significantly effective.”
– Jan Berger, M.D., chief medical officer at Silverlink Communications, Inc.
Click here to read the DRUG BENEFIT NEWS article in which this quote appeared.
June 6, 2013 0 Comments
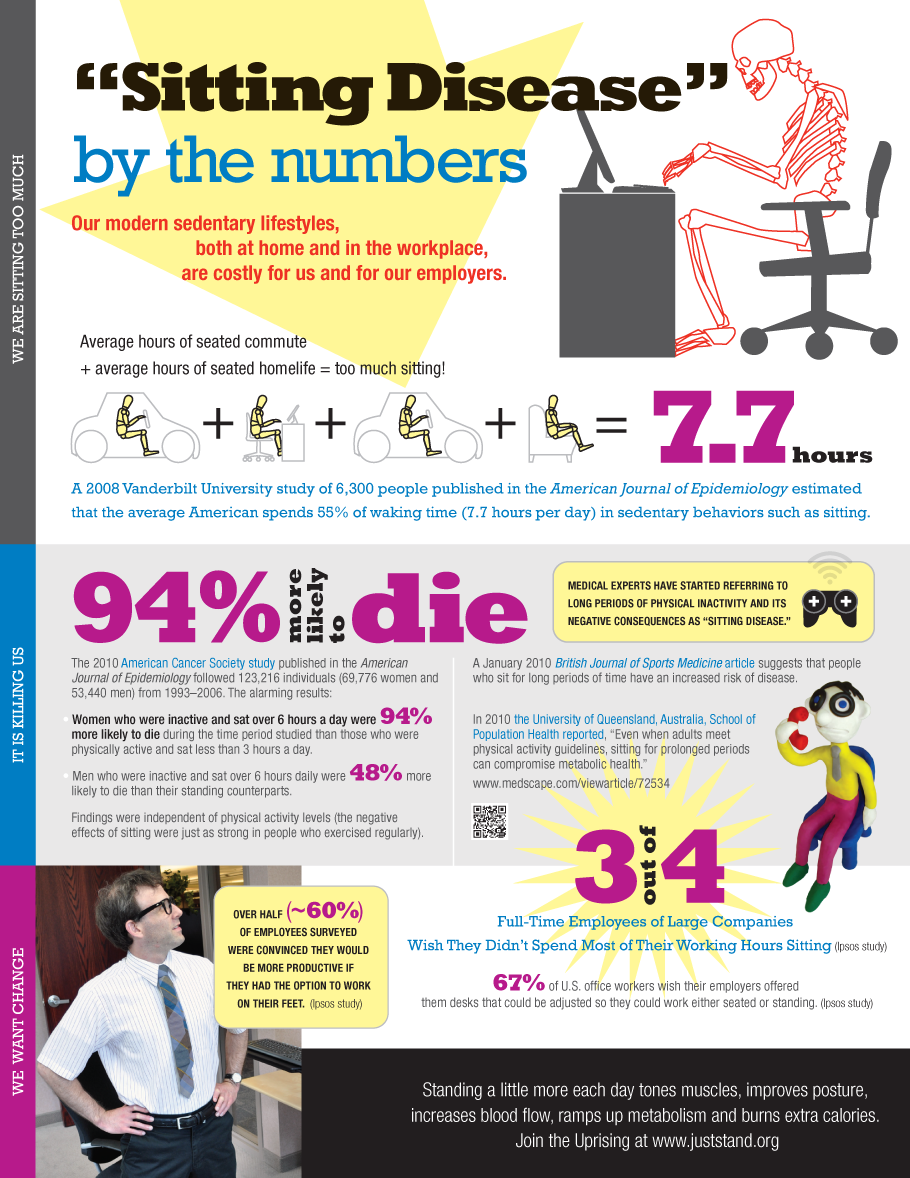
If you haven’t heard, “sitting is the new smoking” in terms of health status. And, unfortunately, you can’t just get up and exercise for an hour and then go sit all day. That brief spurt of exercise doesn’t change the fact that we sit for 9+ hours a day.
If you think about our shift in work from a very manual work environment to a service and technology work environment, we’ve made activity during the day harder and harder to achieve. Between e-mail and meetings, most of us are stagnant to accomplish our work.
That got me thinking about the #QuantifiedSelf movement and all of the activity trackers (e.g., FitBit, BodyMedia). We know companies definitely look online to see people’s social media activity as part of the interview process. Will they begin to ask about their activity data as a proxy for health?
On the flipside, perhaps the person interviewing should really be asking to see their potential boss’ activity data. I’d be as interested in knowing what happens during the day. It would provide a lot of insight into what happens in terms of meetings, face-t0-face activity, and be a good proxy for the real work experience.
Of course, the other option would be to introduce “walking interviews”. People talk about walking meetings. I’ve even done a running meeting going for a jog with a potential partner to discuss how we work together. (It was the only time we could find to meet at a conference.)
Walking interviews would tell you a lot about someone’s health. You could go up some stairs. You could walk a few miles in an hour.
Since we know that health, happiness, and wealth are all correlated, this type of insight for the interviewer and interviewee seems very valuable.
May 22, 2013 1 Comment

Those of you who know me know that I’ve been a huge advocate for generic prescriptions since the early part of my PBM/pharmacy career in 2001. It wasn’t long ago that I talked about unresponsible reporting when slamming generics and scaring the population. But, we all enjoy a good conspiracy theory which is about the only thing that makes sense reading the new Fortune article – Dirty Medicine – about Ranbaxy. Both articles are written by the same author, but this one scares me a lot more than the other one. This article reads like a fiction book but appears to be true. It should scare you also and put a spotlight on the FDA.
Here are a few things from the article.
On May 13, Ranbaxy pleaded guilty to seven federal criminal counts of selling adulterated drugs with intent to defraud, failing to report that its drugs didn’t meet specifications, and making intentionally false statements to the government. Ranbaxy agreed to pay $500 million in fines, forfeitures, and penalties — the most ever levied against a generic-drug company.
The company manipulated almost every aspect of its manufacturing process to quickly produce impressive-looking data that would bolster its bottom line. “This was not something that was concealed,” Thakur says. It was “common knowledge among senior managers of the company, heads of research and development, people responsible for formulation to the clinical people.”
It made clear that Ranbaxy had lied to regulators and falsified data in every country examined in the report. “More than 200 products in more than 40 countries” have “elements of data that were fabricated to support business needs,” the PowerPoint reported. “Business needs,” the report showed, was a euphemism for ways in which Ranbaxy could minimize cost, maximize profit, and dupe regulators into approving substandard drugs.
But, we know that generics have worked. People have gotten better so one has to assume this isn’t a massive fraud especially when 50% of generics have traditionally been made by the brand manufacturers themselves who would never risk their companies to do what Ranbaxy did. So, it made me wonder about the Placebo Effect. Did some drugs work simply because of that? Is there anything else that would make sense for why this wasn’t discovered more quickly?
I’ve talked a lot about the Placebo Effect. There’s now even an app to make you feel better using the Placebo Effect.
I’m shocked that the PBMs, pharmacies, manufacturers, associations, wholesalers, and others aren’t out talking about this. I would want to let the public know that this isn’t a systemic problem, but is one contained to one instance and that quality will be maintained…but maybe no one cares?
May 22, 2013 0 Comments
Surprisingly, I’ve been happily living in the St. Louis area for almost 20 years. I moved here after going to the University of Michigan for graduate school at Washington University, and I never thought I’d stay. My girlfriend (now wife) moved a year later, and we’ve loved it ever since. We’ve built two houses, had two kids, and made a lot of friends.
I’ve had chances to move many times to Kansas City, San Francisco, Boston, Columbia (SC), Florida, Minneapolis, New York, New Jersey, and several other cities. All of them I have turned down. So, one of the big questions I get asked now days is why are you moving out of St. Louis since you’ve commuted for so long and “enjoyed” it. That’s a tough one, but as someone who cares about my health, let me position this from a health perspective for all of you.
Ultimately, we’re moving for one reason which is to spend more time with my family. Of those 20 years, I estimate that I’ve spent at least 9 of them where I traveled 50-90% of the business days. You can do the math, but if I assume 15 days per month on the road over 9 years, that’s about 1,620 days that I’ve been gone or 4.4 years. That’s a lot of time to miss with your wife and kids.
But, I also see several health reasons for this:
Of course, commuting has some productivity gains (if done right) from a work perspective:
You have to trade this off with productivity lost on travel days (e.g., I wake up every Monday at 4:30, leave for the airport at 5:30, land in Charlotte at 10:15, and get to my office around 11:30 with best case 90 minutes of work done).
But, moving definitely impacts your presenteeism as I’m learning (at least for a few months). After 20 years in one city, there’s a lot to do to move. You have to find new service providers (doctors, dentists, handyman, vet, hair), new schools, new sports teams, new stores, etc.
But, for those of you that aren’t convinced since you think travel is glamorous, let me share just a few stories with you.
Of course, the frequent flyer miles and hotel points are great. We’ve taken many a trip with it. I’ve given my parents free flights. Heck, we’ve even given our dog walkers free flights.
The key is to evaluate several factors which are what I’ve looked at:
Anyways, this has been one reason why I haven’t been blogging as much lately. The move is all consuming especially with lots of things going on at work. I have 4 more days in St. Louis before moving so we’re excited and nervous.
May 18, 2013 0 Comments
Guest Post From The President of TeleVox Software
It shouldn’t come as a surprise to anyone that we live in a society yearning for instant gratification. We expect to get information in the blink of an eye, the answers we need within minutes and material goods delivered prior to the date that was promised. But what may surprise you is that even through the desire to have this information so quickly, the importance of providing a personalized message remains one of consumers’ biggest wishes. For instance, studies show that tailoring the message to the needs of patients as well as personalizing the messages are key to successful high-tech patient engagement. In fact, according to a recent TeleVox Healthy World Report, Technology Beyond the Exam Room: How Digital Media Is Helping Doctors Deliver the Highest Level of Care, 50 percent of patients expect information to be personalized to their specific needs. In the age of instant feedback and heightened technology, it is interesting to know that patients still desire a personalized approach in terms of their healthcare.
The days of simply setting forth wellness plans based solely on numbers and stereotypes are past us. Patients are looking for communications that are relevant to their lives, and it is their expectation that healthcare professionals will take time to engage in this level of personalization. Know Your Health also found that 53 percent of patients expect communications to be relevant to them as individuals. Relevant patient engagement can include personalized interactions, individualized treatment plans, and follow up. Patients thrive on a feeling of importance, ranging from a doctor knowing their name and medical history when they walk in to a follow-up call or email after the appointment to continue that personal connection.
Think about this: According to the same report, 21 percent of the population will refuse information if it is not tailored specifically to them. And, further, 13 percent of patients surveyed report they will ignore information sent their way if it doesn’t have their name on it. Why would providers want to miss out on connecting with an important part of the population by simply not including their name on any communication to the patient? Including this step can ensure patient engagement is successful and save valuable resources, as the information conveyed will have a better chance of being received by patients.
Finally, taking time to connect with patients outside of their yearly exams or scheduled check-ups is another important link in ensuring that patients make positive decisions that ensure a healthy future. 68 percent of the population would like to receive educational tips that will help them live a better life via email throughout the year. Many Americans are concerned with the direction of the overall health and well-being of the country, but still aren’t taking steps to get where they need to be. However, healthcare providers can take steps to tailor messages that are relevant and personalized to patients to ensure successful high-tech patient engagement, and ultimately a healthier America.
Scott Zimmerman is a regularly-published thought leader on engaging patients via ongoing communication between office visits. He is the President of TeleVox Software, Inc, a high-tech Engagement Communications company that provides automated voice, email, SMS and web solutions that activate positive patient behaviors by applying technology to deliver a human touch. Scott spearheads TeleVox’s Healthy World initiative, a program that leverages ethnographic research to uncover, understand and interpret both patient and provider points of view with the end goal of creating a healthy world–one person at a time. Zimmerman possesses 20 years of proven performance in the healthcare industry, with domain knowledge in the surgical, interventional and pharmaceutical arenas. Prior to joining TeleVox, Scott served for nine years at GE Healthcare in a variety of cross-functional and global leadership roles in sales, services, quality, marketing, pricing, finance and product development. Scott is a graduate of the John M. Olin School of Business at Washington University in St. Louis.
May 6, 2013 5 Comments
I think we all know that medication adherence is a big deal. The most common number quoted is the $290B waste number from NEHI. There are numerous studies that confirm the value of non-adherence even one that just came out.
The amount of money spent on trying to improve adherence is huge! Pharma has worked on. Retail pharmacies have worked on it. Providers have worked on it. Insurance companies have worked on it. Employers have worked on it… And all of these have happened across the world.
At the same time, you see people get so excited about things don’t make any sense to me.
Let me take an easy example. A few months ago, a company called MediSafe put out a press release around moving medication adherence on statins up to 84.25%. Nothing against the company, but I read the press release and reached out to them to say “this is great, but it’s only 2 months of data…most people drop therapy after the first few months so who care…call me back when you get some good 12 month data.”
But, a lot of people got all excited and there was numerous press about this – see list of articles about them.
Now, tonight, I see another technology getting similar excitement. Fast Company talks about the AdhereTech technology which integrates a cellular phone with a pill bottle. And, it costs $60 a month. In my experience, companies wouldn’t even spend $2 a month to promote adherence so $60 is just impractical. The argument is that this is good for high cost specialty drugs that are oral solids not injectables. But, this isn’t a new idea. Glowcaps already built this model with a very slick interface and workflow.
And, I don’t know about you, but I think this would be obnoxious. And, I love data and am part of the QuantifiedSelf movement. I’m not sure I understand the consumer research here. I would have to believe all of the following to buy into this model.
Yes. Will this work for some people…sure. But, if it helps 10% of people, then my cost is really $600 per success.
Should we be working on better solutions to address adherence…of course.
But, let’s stop trying to figure out some gimmick to fix adherence. Let’s look at root cause.
For example:
We have a lot of problems.
May 6, 2013 0 Comments
I must admit that I don’t remember taking the presidential fitness test as a kid. With that being said, I was surprised to learn from my daughter that in her class of club soccer, volleyball, and baseball players she was the only kid to meet the highest level (greater than the 85th percentile across several measures). She made it today by running her mile in 7:37.
So, what does this require? It made me curious. Here’s what you have to do:
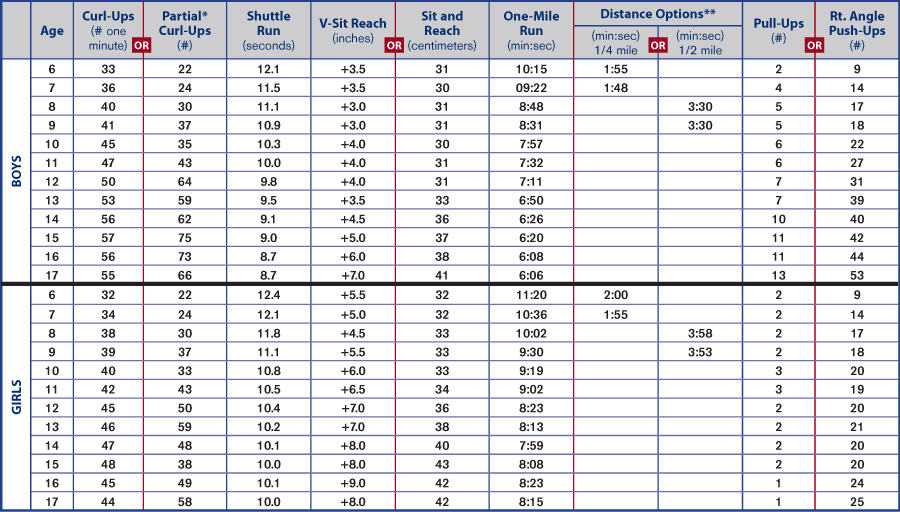
Could you do that? These seem pretty difficult to me. I could probably do the mile in 6:06, but I doubt I could do 53 pull-ups. And, I doubt I could sit and reach 7 inches beyond my toes. (Looking at the 17 year old male standards.)
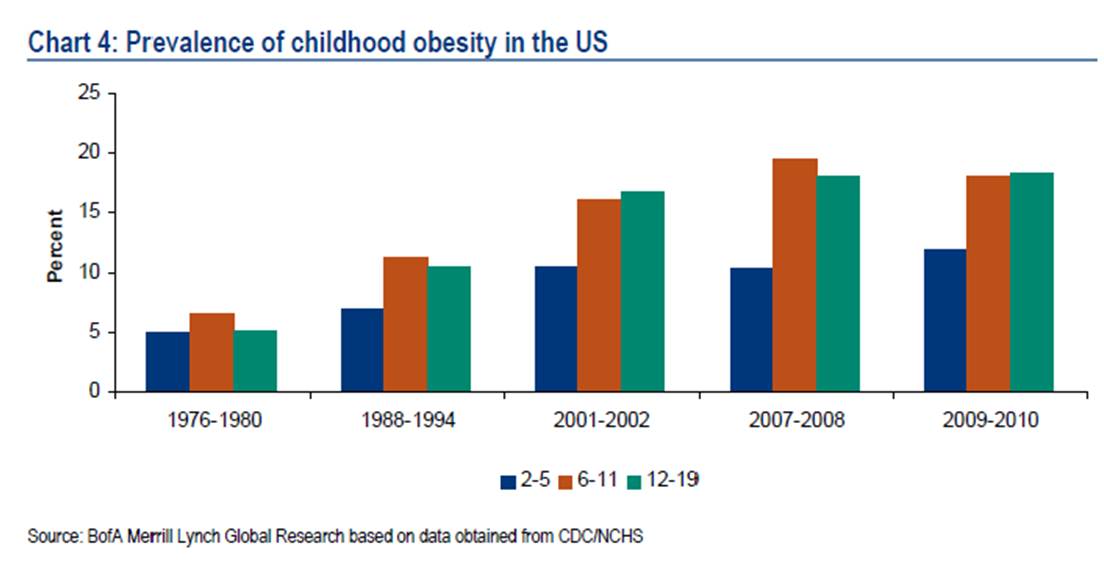
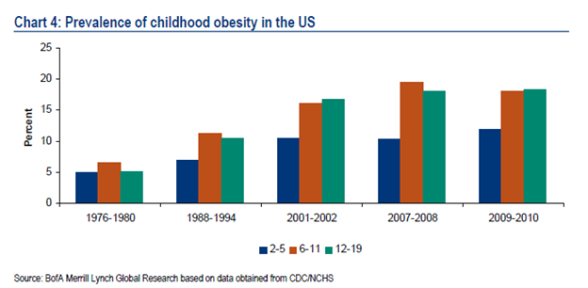
On the other hand, we certainly need our kids to be more fit. We have a big childhood obesity issue.
But, it also made me think about Michelle Obama’s efforts in this space.

I think these programs are good starts, but lets not forget that obesity is a social issue and kids learn from those around them. Let me ask the uncomfortable questions about those who our kids look up to.
These are all key role models…not to mention us parents who are often overweight.
I guess my suggestion here to the President would be to think about how to use our massive government payrolls as a foundation for change. Let’s think about the Presidential Fitness Challenge and create a broader wellness solution to change the visual role models for our kids and figure out how to help companies invest in this.
For example, we know that sleeping is correlated to weight and health. I was talking to my brother-in-law who is a police officer when he told me that they are expected to get 8 hours of sleep a night. Imagine if companies set this expectation for their employees (sleep impact on work).
“Sitting Disease” may make a great late night comedy story line, but it’s a reality of our information economy that has to be addressed.

April 28, 2013 3 Comments
While we are generally a society focused on innovation from start-ups (and now all the incubators like Rock Health), there are a few big companies that are able to innovate while growing. That’s not always easy and companies often need some catalyst to make this happen. Right now, there are four established healthcare companies that I’m watching closely to track their innovation – Kaiser, United/Optum, Aetna, and Walgreens. (Walgreens has made the Fast Company innovation list 3 of the past 4 years.)
I think Walgreens is really interesting, and they did have a great catalyst to force them to really dig deep to think about how do we survive in a big PBM world. It seems like the answer has been to become a healthcare company not just a pharmacy (as they say “at the corner of Happy and Healthy”) while simultaneously continuing to grow in the specialty pharmacy and store area.
Let’s look at some of the changes they’ve made over the past 5 years. Looking back, I would have described them as an organic growth company with a “not-invented-here” attitude. Now, I think they have leapfrogged the marketplace to become a model for innovation.
“Today’s announcement marks another step forward in establishing an unprecedented and efficient global pharmacy-led, health and wellbeing network, and achieving our vision of becoming the first choice in health and daily living for everyone in America and beyond,” said Gregory Wasson, President and Chief Executive Officer of Walgreens. “We are excited to be expanding our existing relationship with AmerisourceBergen to a 10-year strategic long-term contract, representing another transformational step in the pharmaceutical supply chain. We believe this relationship will create a wide range of opportunities and innovations in the rapidly changing U.S. and global health care environment that we expect will benefit all of our stakeholders.”
“With this service expansion, Take Care Clinics now provide the most comprehensive service offering within the retail clinic industry, and can play an even more valuable role in helping patients get, stay and live well,” said Dr. Jeffrey Kang, senior vice president of health and wellness services and solutions, Walgreens. “Through greater access to services and a broader focus on disease prevention and chronic condition management, our clinics can connect and work with physicians and other providers to better help support the increasing demands on our health care system today.” (from Press Release)
This is something for the whole pharmacy (PBM, pharma, retail, mail, specialty) industry to watch and model as I talked about in my PBMI presentation (which I’m giving again tomorrow in Chicago). It reminds me of some of the discussions by pharma leaders about the need to go “beyond the pill”.
April 9, 2013 0 Comments
Do you know the term “pivot“? It’s all the rage now in terms of describing how companies continue to evolve their models with this rapidly changing business environment.
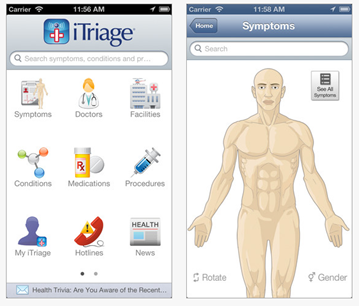
Of course, Aetna is one of the big healthcare players in the US. They’re not going to abandon a model that’s been working for well over 100 years. But, thanks to some great leadership from people like Mark Bertolini, CEO of Aetna, they’ve created a new business unit called Healthagen (building on the company they bought known mostly for iTriage). The screen shot says it all.

I got the privilege to sit down with Dr. Charles Saunders who runs Healthagen at the World Healthcare Congress in DC (#whcc13).
Charles E. Saunders, M.D., is responsible for leading the strategic diversification of Healthagen’s products, services and global opportunities. He focuses on identifying new growth opportunities and developing market strategies that can help Healthagen and Aetna profitably manage quality and cost for its customers.
Prior to joining Healthagen, Dr. Saunders served as executive in residence at Warburg Pincus, one of the world’s largest and oldest private equity firms. He has held a number of other significant leadership positions during his career, including CEO of Broadlane, Inc., President of EDS Healthcare Global Industry Solutions; Chief Medical Officer of Healtheon / WebMD; Principal of A.T. Kearney; and Executive Director of San Francisco General Hospital Managed Care Programs.
Dr. Saunders received a B.S. in biological sciences from the University of Southern California and an M.D. from Johns Hopkins University. He is board certified in Internal Medicine and Emergency Medicine and has served on the faculty of several universities, including the University of California, San Francisco; Vanderbilt University; and University of Colorado.
I also got to hear him speak right before I talked to him. (As a side note, he is a great presenter which is something that I really respect in a world of people who present too many slides, use notes, talk to the screen, and can lose you quickly.)
He hit on several key themes in his presentation that we then discussed further face-to-face:
One of my first questions was to really understand Healthagen and what it was set up to do. (As you can see from the screen shot below, they’re doing lots of things in this group.)

He boiled it down nicely to three things:
Our next discussion was really around why and how to create and innovate within a large company like Aetna. He reiterated what I believed that Mark Bertolini championed this new vision along with several of the other senior leaders. But, I think the key was that they recognized that issue of trying to do that internally and were willing to form a group to be different. To minimize bureaucracy for this group. And, to leverage their capital and assets to support this group. Not many big companies do this well. My impression is that Aetna is and will continue to be successful here. (Full disclosure – I own a minor number of Aetna shares and have believed this since I bought them about a year ago.)
Of course, in today’s market, there’s an explosion of innovation with questions on the short-term and long-term ROI of many initiatives and start-ups. With that in mind, Dr. Saunders pointed out that they don’t want to own everything. They want to create a plug and play platform of enablement. iTriage is a great example of this where they brought in a mobile technology with 2M downloads in 2011 and now have over 9.5M downloads of the tool (on top of massive increases in functionality and integration). You can download it here – https://itunes.apple.com/app/itriage-health-doctor-symptoms/id304696939?mt=8.
Certainly, one concern others have historically had in this space was how to own solutions and sell them to their peers (competitors). Dr. Saunders talked about their ability to do this with ActiveHealth and a perception that the industry is over that issue as long as Aetna can continue to demonstrate that they are good stewards of the data and are keeping the appropriate firewalls in place.
We wrapped up the conversation talking about the social caregiver and game theory. I think both are important in our mHealth / digital world. With the sandwhich generation, this is increasingly important. That is where Aetna is focusing…enablement of the caregiver for infants and seniors leveraging a social approach. This reminds me of their recent announcement of a pilot with PatientsLikeMe. We also talked about game theory and the role of that in healthcare which is a common theme from my discussion with Keas this morning and a theme from the overall conference.
It should be interesting to watch Dr. Saunders and his team and how Aetna continues to pivot.
April 9, 2013 0 Comments
I’m at the World Healthcare Congress (WHCC13) in Washington DC this week. This has always been one of the top 5 events for me to try to come to every year (admitting that there are a few like TED that I haven’t attended due to budget yet).
It’s interesting how trends start to flow within a conference and how the trends change year to year. This year, the key themes that I continue to hear are (in no order):
But, since Twitter is my new note taker…here’s a few sets of tweets for you.


April 9, 2013 0 Comments

I had the opportunity to sit down this morning with Josh Stevens who is the CEO of Keas.
“Keas is the most engaging wellness program in the workplace. Keas promotes healthy behavior and teamwork with interactive media that delivers relevant, individualized content to hundreds of thousands of employees. Keas has a proven track record of supporting corporate HR in increasing retention, productivity, teamwork, collaboration, and competitiveness. By rewarding people for achieving simple exercise and nutrition goals, employee health is improved and overall healthcare costs are decreased.”
He is a passionate believer in using fun and social to drive change in healthcare with a focus initially on wellness and then moving upstream to other challenges like disease management.
As CEO of Keas, the market leader in corporate wellness, Stevens is responsible for leading the development and market adoption of the company’s breakthrough wellness platform and applications.
Stevens has over 20 years of experience in product, sales, marketing, and is a recognized leader in driving high-value product experiences that deliver customer delight and investor’s valuation growth.
Prior to Keas, Stevens was Vice President of e-commerce at YouSendIt, Senior Vice President of strategy and business development at TicketsNow, and General Manager of e-commerce at AOL. Prior to his GM role at AOL, Stevens held a variety of leadership positions in business development, product marketing, product management, and corporate strategy.
Some of you may have seen Keas over the years. They were founded by Adam Bosworth who was responsible for Google Health at one point. They’ve gone through a few evolutions, but it seems like they’ve hit on a working model leveraging several principles that we discussed:
While Josh isn’t a healthcare native, that seems like a good thing. I’ve seen a lot of people try to come into healthcare from the outside. Most of them fail because they get overwhelmed by the regulation or frustrated by the challenges or stick too much to what they personally think should work. In the hour we spent together, I didn’t get that sense.
I’m looking forward to learning more about Keas and trying out the tools myself. One of the most fascinating points was that they get people to engage 15 times per month. I told him that that was a ridiculous number in healthcare. We went on to talk about his hiring a team from the gaming industry and that they were used to being tied to repeat visits not simply getting people to download the tool.
IMHO – if you could get 50% of people to engage twice a month with a tool (and sustain that engagement rate), you would be a hero.
As I’ve talked about in my posts about CVS and as I tweeted earlier today from the conference, companies need to engage the worker at the workplace to transform healthcare. Josh gets that key point.
“Today’s employees spend most of their daily lives at work and companies can have a huge impact on improving overall health by creating a culture of wellness at work. That culture starts with Keas’ fun, engaging platform, which helps employees become healthier, more productive and more engaged at work, and in life.” (press release)

March 30, 2013 0 Comments
I continue to annoyed by all the fear-mongering in the industry around what CVS Caremark is “doing to their employees”. What about focusing on how they are helping their employees to get better? (If interested, you should read some of the information they have on their blog.)
Our “Plan for Health” combines an evolving, best-practice approach to health coverage with preventive care and wellness programs. Our colleagues will be more accountable for taking control of their health and associated costs. The first step is getting to know your numbers by getting a health screening and completing an online wellness review each year. If colleagues complete both by the May 1, 2013 deadline, they will avoid paying an additional $600 for the 2013-2014 plan year. (from the CVS Caremark blog)
I was hopeful to hear someone come out strongly and speak about it yesterday on CBS, but instead the CEO of Mercer just talked about “soft” programs that depend upon consumers being proactive around their health. I would rather hear about the value of screenings and how it helps employees. In talking with one friend of mine at a biometrics company, he told me that in one case almost 40% of the people that they identified with diabetes (or pre-diabetes) and hypertension (or pre-hypertension) didn’t know they had the disease (or were at high risk). That to me is a valuable insight to the individual especially when coupled with a program to help them learn and manage their disease (or risk).
For example, companies for years have been using Health Risk Assessments (HRAs) to try to baseline employee health and use that to accomplish several things:
Use of biometrics is the right evolution from the HRA. People have tried HRAs for years with some success. Companies pay as much as $600 for people to take this online survey that has no necessary link to reality. Most HRAs aren’t linked to lab values. Most HRAs aren’t linked to claims data. Most HRAs don’t necessarily trigger enrollment in health programs. They are supposed to activate the employee to be proactive which doesn’t work for many sick consumers especially those in the “pre-disease” phase. (Here’s a good study that does show some increased activation.)
As I mentioned the other day, this use of biometrics and link between incentives and participation (and ultimately outcomes) is normal and will ultimately improve the link between the workplace and the employee around health.
Let’s take a broader look at insurance to help set some context:
Whether we want to admit it or not, we do determine a lot of our healthcare costs based on decisions we’ve made or had made for us since we were kids. Some of these are conscious and some are subconscious. And, obesity which is a large driver of many of these chronic conditions and has an impact on your likelihood of having cancer. So, a company asking for your BMI and other data to help understand your risks for healthcare costs (of which they typically pick up 80%) doesn’t seem unusual.
Certainly, some are environmental such as those that live in “food deserts” like Detroit. In other cases, workplace stress can affect our health. We’re just starting to get smarter about “sitting disease” and it’s impact on our health. Or, we may take medications that affect our blood pressure (for example). It’s certainly important to understand these in context of your lab values and discuss a holistic strategy for improving your health with your physician and any care management resources which are provided to you (nurse, social worker, nutritionist, pharmacist).
This idea of learning more about employees in terms of biometrics, food, sleep, stress, social interaction, and many other data points is going to be more and more of a focus. Companies want to learn how their employees do things. They want to understand their health. They want to improve their health. They want to invest in their workforce to improve productivity, innovation, and ultimately job satisfaction.
While the glass half-empty people won’t see this and there are some companies that don’t always act this way, I generally believe that companies are trying to act in a way to increase their top line and most intelligent executives understand the correlation between health and wealth and the link between employee satisfaction and growth.
Ultimately, healthcare costs are estimated to put a $240,000 burden on us after we retire (even with Medicare) so if someone wants to help me become healthier and thereby save me money which improves my ability to retire and enjoy life I’m happy for them to do.
March 25, 2013 1 Comment
No…this is not about how Google Glass can impact healthcare although I do believe it can and will (something many are talking about).

This is about how the QuantifiedSelf movement can change your view of the world. Ever since I’ve been using the FitBit (see my review) and focusing on getting 10,000 plus steps per day, I’ve noticed a change in how I view the world.
Here’s some examples:
It’s a totally different way of thinking about life when you look through these “quantified self glasses” to see the world through a “health lense” about calories, exercise, sleep, stress, and other dimensions.
March 22, 2013 1 Comment
Have you heard that CVS Caremark is requiring employees to go get biometrics and going to take action on it? OMG!
I’m not sure I understand why people are all upset. Let’s look at the facts:
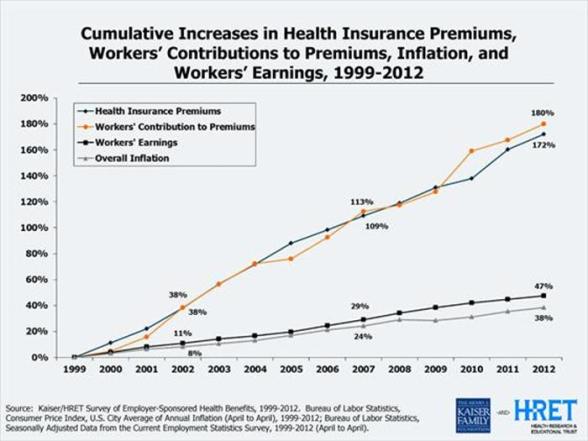
And, by the way, have we forgotten how much healthcare costs have gone up over time and who pays that bill. It’s either the employer or the government. Both of those things impact our pay as individuals either in terms of lower raises to cover healthcare costs, shifting healthcare costs to us, or taxes. It’s not sustainable so the person who pays the bill has to step in since we’re not. (Which is also why I support the NY ban on soda.)
Now, let’s look at our healthcare system where in the current fee-for-service model, there isn’t an incentive for physicians to address this.
For now, people should be happy. They’re only being required to do the biometrics. The penalty isn’t linked to whether they’re fat or have high blood pressure or smoke or have high cholesterol or have diabetes. A recent study by Towers Watson shows that while 16% of employers do this type of outcome based incentive program today (2013) that this is going to jump to 47% in 2014. So, this will be the norm.
And, guess what…sticks often work better than carrots in some cases.
And, healthcare costs are making us uncompetitive globally as a country.
And, health reform is allowing (even enabling) this to happen. It says that you can treat people differently and create up to a 50% differential in costs associated with their health. (Not a legal definition so read the fine print.)
But, what I think all of us (consumers and employers) will need to realize is that moving to this (which I agree with) will change the employer and employee relationship in several ways.
If none of this motivates you, then just think about the “gift” we’re giving our kids and maybe that will be a wake-up call why someone has to do something here. (As I shared the other day, I struggle with my weight so don’t think I’m some super skinny, high metabolism person who thinks this is easy.)
March 20, 2013 0 Comments
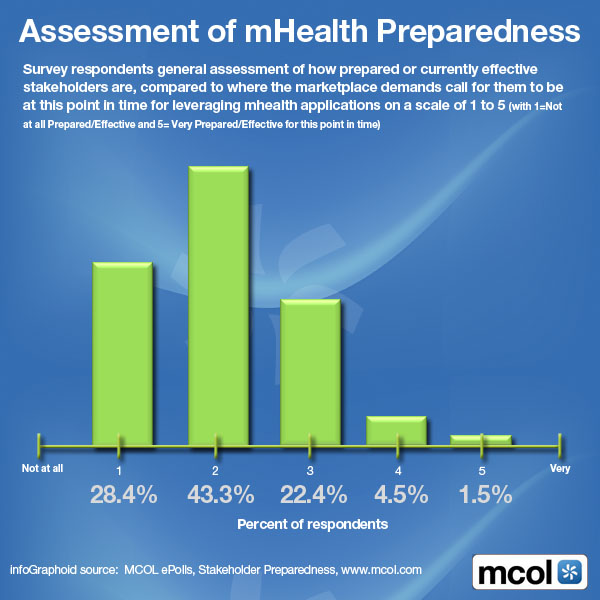
The data from these two surveys just passed my desk so I thought I would post them.

March 20, 2013 0 Comments
I’ve being doing a lot of work lately on how to tackle the obesity problem in the US. This has been great personally as it has forced me to look at lots of research to understand all the tools out there.
It’s also made me look at different drivers of obesity including sleep and stress. The new report out showing that sitting is a huge problem (even if you exercise) is very eye-opening also.
For years, I’ve talked about my challenges is managing my weight which lead to some fluctuations, but at the end of the day, I think a lot of this boils down to a “Golden Moment” or a “Moment4Change”. Even people who do this every day (e.g., doctors or sports coaches) are often overweight. We have to have something which prompts us to change our life. We aren’t generally motivated by dropping our HDL. We’re motivated by being able to play with our kids or living long enough to see our kids get married.
In my life, there have been several Moment4Change points so I thought I would put this out there to hear what’s motivated others:
So, I’m interested. What has motivated you to changed? And, how do you measure success? I suggested that while women may use the “skinny jeans” test that men might be more likely to use the “belt buckle” test.
RT @gvanantwerp: Is the male equivalent of the #skinnyjeans test the #beltloop test?#quantifiedself #mhealth cc @susannahfox
— healthythinker (@healthythinker) March 14, 2013
I think this image below from the AON Hewitt 2012 Health Care Survey is a good one about the fact that 80% of our costs are driven by 8 behaviors.

I also thought that this presentation at the FMI by The Well which was a GSW project was right in line with this.
March 17, 2013 0 Comments
We all talk about the challenge of consumer engagement in healthcare. If we can’t get consumers to engage, we’ll never get them to change behavior or be preventative.
But, as the recent Times article highlights, sometimes engagement still leads to failure which can be very frustrating. As I think about my recent experience within the pharmacy system, I’m reminded of a comment that I re-tweeted yesterday.
@reginaherzlinger asks why you need to have connections to get clear information about cost and quality if care.
— Liz Boehm (@LizBoehm) March 16, 2013
In this case, I have connections which I suppose I could escalate this to, but it seems wrong that the only way to resolve my customer service issue is to call in personal favors from Express Scripts and CVS.
@expressscripts #rx #fail. Refill rejected due to @cvs refill I never picked up 3 mo ago. Why is it my issue 2 resolve?Call pharmacy #cx
— George Van Antwerp (@gvanantwerp) March 9, 2013
But, maybe that’s what I’ll have to do. At this point, the only way I seem to be able to get my medication is to pay cash which seems like a total system failure. (Thankfully, I can use the GoodRx app to figure out which pharmacies have the lowest cash price for me.)
So, here’s the scenario…
Who knows when this will resolve itself, but everyone seems to be able to blame someone else here. Never mind that the patient (me) can’t get their medication. As someone who tries to look at this from the average consumer’s perspective, this is a nightmare and total customer experience failure. I understand the system. I understand plan design. I know the pharmacists. I know the teams at Express Scripts and CVS. Even with all that, I’m stuck having to go outside the system, pay cash for my prescription, and hope that my paper claim will get processed and hit my deductible in my plan design.

March 12, 2013 1 Comment

There are lots of fundamental issues here:
At the end of the day, I look at it very differently. I think the proposed ban was great. I was very annoyed last night to find out it was overturned.
Why?
So, enjoy your big 64 oz soda now, but when you’re 69 and Medicare has been rolled back to 70 due to funding challenges, you can smile and remember that you got to enjoy all that sugar for years without anyone trying to help you. (I can picture a great political cartoon here of the patient getting a healthcare bill looking over their shoulder from their wheelchair to see a big pile of soda cups!) Never mind the fact that you’re bankrupt due to your healthcare bills and not able to walk around to keep up with your grandkids.

Source: top-nursing-programs.com
March 11, 2013 1 Comment
I spend a lot of my personal and professional time trying to figure out how to better engage consumers in healthcare. If you can’t engage them, you can’t improve outcomes.
Never mind the fact that people experience about 5,000 messages a day so you have to cut through that clutter.
Even if we do cut through the clutter, people are busy living their lives. They’re worried about their family. They’re worried about the economy. They’re trying to keep food on the table. They are generally overwhelmed with too little sleep and too much stress.
But, let’s even assume that you can cut through the clutter and get them to listen, you still struggle with getting a person at a time when they are open to change. These “golden moments” require them to see value in the change and feel like the short-term effort is worth the long-term gain. This “value exchange” doesn’t often exist. And, with 30% variance in the healthcare system, people often don’t trust the system.
Even with all that in mind, people still don’t engage. They don’t get flu shots. They don’t fill their medications. They don’t understand the messages that are delivered to them.
Here’s a quick image I created for a presentation later this week.

A few of the sources for this are:
March 4, 2013 0 Comments
“In our modern effort to eradicate disease, we pop antibiotics like candy, apply hand sanitizers with abandon, and gargle mouthwash by the gallon. But this carpet-bombing of germs takes a huge toll on good microbes as well as bad. The March/April issue of The Saturday Evening Post, on newsstands now, reveals recent research pointing to medical problems including asthma, obesity, and chronic sinusitis that might be caused by the absence of certain microbiota in our bodies.” (From a press release about the article Why We Need Germs.)
What if the bacteria in our body was a determining factor in chronic conditions? Would you try to get more bacteria into your body? Would you stop doing things to kill the bacteria? Would this change our eating habits?
This is a fascinating article by The Saturday Evening Post, it shares some research that might explain why two people can have the same food habits and one be skinny and one be fat. (A frustrating thing for many of us.)
You can even learn about a crowdsourcing project that will take your feces and tell you the bacteria in your gut.
In the meantime, you might want to eat more asparagus and garlic. Yummy! And, be less stressed out.
For instance, Bacteroidetes—the microbes linked to slimness—proliferate in the presence of fructans, a form of fructose found in asparagus, artichokes, garlic, and onions, among other foods, notes microbiologist Andrew Gewirtz of Georgia State University. A diet high in fructans might support a good crop of slimming Bacteroidetes. On the other hand, he notes, stress decreases the abundance of Bacteroidetes, suggesting one more way stress causes obesity.
March 2, 2013 0 Comments
The fact that most people would rate their experience with their health insurer low isn’t a big surprise to most of us in healthcare. But, with the Triple Aim and other quality metrics, the customer experience is becoming an increasingly important metric. Several recent surveys have talked about this as one of the top priorities for hospital systems. And, as use of CAHPS continues to grow, this will be more closely linked with incentives.
“Patient experience is on the radar of hospital executives, especially since Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores will soon affect reimbursement,” said Jason Wolf, executive director of the Beryl Institute. “However, the data shows that executives are still grappling with how to implement change within their organizations.” (source)
Like in years past, health insurers just barely nudge out TV service providers to prevent being the bottom of the industry in Bruce Temkin’s Benchmarking work. While I’d love to see healthcare broken out into hospitals, physicians, pharmacies, insurance companies, PBMs, and care management companies, I think we can assume some similar concerns would fall out.
Healthcare companies need to find ways to address this. I think there are several key first steps:


February 26, 2013 0 Comments
I was monitoring a pharma conference over in Europe this morning. I found a few of the dialogues really interesting. One of them was about a company creating all these websites to allow consumers to engage with them. There was then some debate.
It’s not about the channel it’s about the strategy #digpharm
— Samantha Collings (@SamCollings) February 26, 2013
@chrisschulze I agree. Having websites isn’t a digital strategy. That’s a pre-2000 strategy. #digpharm
— George Van Antwerp (@gvanantwerp) February 26, 2013
On the on hand, I can agree that you can do some creative things with the channel, and therefore, I should be too down on someone who is very web centric. (i.e., focus on the strategy) On the other hand, digital is much bigger than web.
I’m sure there’s a lot of views here, but let me share mine in terms of what to consider from a digital strategy:
While there are a lot of complicated images out there trying to show everything around digital strategy, I found this one pretty simple and concise.

February 26, 2013 0 Comments
As I’ve been looking at the employer view of healthcare, it strikes me that there are two different fundamental approaches.
Unfortunately, this likely means that the most vulnerable population is disadvantaged in this model (i.e., the hourly worker who is in a job where they are easily interchanged with another employee).
But, for companies where their biggest asset is their people (e.g., Microsoft), it seems clear that they would want to focus on healthcare as an investment.
This might drive you to make different decisions.
It seems like you would look at these types of decisions differently. It wouldn’t be about the lowest healthcare premium. It wouldn’t be about pushing them to a limited network. It wouldn’t be about limiting their choice. It wouldn’t be about shifting costs. It would be about guiding them to make choices that kept them happy, productive, and engaged so that they could do the best work for you.
This would involve addressing stress. It would involve addressing sleep patterns. It would involve helping them create a work-life balance.
February 24, 2013 0 Comments
I was finally catching up on my Biggest Loser shows yesterday. They talked about the Body Peace Treaty from Seventeen magazine. Not something I read, but there are some good points in the treaty. Here are a few for you.
So, while some of the things on the list may be more biased towards young women, the fundamentals are the same for all of us.
February 22, 2013 0 Comments

This is the 3rd time in my life that I’ve lost over 10% of my body weight. I’ve tried it with all exercise. I’ve tried it with all diet changes. And, this time, I think I’ve gotten smarter and am doing it with a combination of both thanks to technology which is helping me to track calories in and out. I try to work towards a 500 calorie deficit every day.
With that in mind, here’s a few lessons learned.

February 19, 2013 0 Comments
Today, I’m giving my presentation at the PBMI conference in Las Vegas. This year, I choose to focus on the idea of shifting from fee-for-service to value-based contracting. People talk about this relative to ACOs (Accountable Care Organizations) and PCMHs (Patient Centered Medical Homes) from a provider perspective. There have been several groups such as the Center For Health Value Innovation and others thinking about this for year, but in general, this is mostly a concept. That being said, I think it’s time for the industry to grab the bull by the horns and force change.
If the PBM industry doesn’t disintermediate itself (to be extreme) then someone will come in and do it for them but per an older post, this ability to adapt is key for the industry. While the industry may feel “too big to fail”, I’m not sure I agree. If you listened the to the Walgreens / Boots investor call last week or saw some of things that captive PBMs and other data companies are trying to do, there are lots of bites at the apple. That being said, I’m not selling my PBM stocks yet.
So, today I’m giving the attached presentation to facilitate this discussion. I’ve also pre-scheduled some of my tweets to highlight key points (see summary below).

February 12, 2013 0 Comments
I just came across this survey data from January of 2010 where the Midwest Business Group on Health (MBGH) did a survey of physicians. I found it really interesting. Let me pull out a few points with some comments…
| The study went on to say that physician’s want employers to provide support around weight loss, smoking cessation, flu shots, and other broad programs. They also want the employer to focus on lifestyle change and health improvement not the chronic disease itself. This makes sense, but in general employees are more focused on trusted information coming from their physician not their employer so there’s a clear gap here. (See graph from Aon Hewitt’s 2011 Health Care Survey, New Paths. New Approaches.)
|
February 11, 2013 1 Comment
12 Of 23 Companies
As I mentioned a few weeks ago (2/2/13), I wanted to test and see if healthcare companies would respond to consumers via Twitter. To test this, I posted a fairly general question or message on Twitter to see the response (see below). Of the 23 companies that I sent a message to, only 12 of them ever responded even after 6 of them received a 2nd message. Those results are shared below. What I also wanted to look at was the average time to respond along with which group was more likely to respond.
I will admit to being surprised. I’m sure all of these companies monitor social media so I’m not sure what leads to the lack of response. [I guess I could give them the out that I clearly indicated it was a test and provided a link to my blog so they could have chosen not to respond.]
Regardless, I learned several things:
From a time perspective, I have to give kudos to the Prime Therapeutics team that responded in a record 2 minutes. Otherwise, here’s a breakout of the times by company with clusters in the first day and approximately 2 days later.
| Company |
Response Time (Hrs:Min) |
| Prime Therapeutics |
0:02 |
| Aetna |
1:12 |
| LoseIt |
1:19 |
| Healthways |
2:07 |
| Walmart |
3:01 |
| Express Scripts |
8:35 |
| Kaiser |
29:22 |
| BCBSIL |
47:32 |
| OptumRx |
47:39 |
| BCBSLA |
48:18 |
| Sanofi |
53:30 |
I guess one could ask the question of whether to engage consumers via Twitter or simply use the channel more as a push messaging strategy. The reality is that consumers want to engage where they are, and there are a lot of people using Twitter. While it might not be the best way to have a personal discussion around PHI (Protected Health Information) given HIPAA, it certainly seems like a channel that you want to monitor and respond to. It gives you a way to route people to a particular phone number, e-mail, or support process.
As Dave Chase said in his Forbes article “Patient engagement is the blockbuster drug of the century”, this is critical for healthcare companies to figure out.

The CVS Caremark team told me that they actively monitor these channels and engage with people directly. I also talked with one of the people on the Express Scripts social monitoring team who told me that they primarily use social media to disseminate thought leadership and research, but that they actively try to engage with any member who has an actionable complaint. They want to be where the audience is and to quickly take the discussion offline.
If you want to see the questions I asked along with the responses, I’ve posted them below…










