May 30, 2008
May 30, 2008 
12 US research groups were awarded grants this week in order to conduct studies on how interactive video games affect players’ health. There has been a lot of press lately for Nintendo Wii and its many health benefits. It seems that the Wii isn’t the only gaming system to influence a person’s lifestyle choices where health is concerned. Of course, not all games are having a positive influence.
Grants totaling up to $200,000 were given to each research team, all of which are connected with a major US university. The generous donations come from Robert Wood Johnson Foundation (RWJF), a private foundation that is dedicated to improving the health of all Americans.
In regards to the grants, RWJF program officer Chinwe Onyekere stated:
We have been actively working in this area since 2004. Over this time, we have heard repeatedly that there is a need for stronger evidence that games can improve health and healthcare and support the growing realization that games can make a real difference in public healthcare in the United States.
Our vision is that in the coming years we will have a thriving marketplace of well designed, compelling interactive games that draw on this evidence base to become highly engaging and effective tools for improving the health and healthcare of Americans.
The 12 teams are currently working on projects that focus on different age groups and behaviors. Maine Medical Center, for example, was awarded a grant for its study, “Family-Based Exergaming with Dance Dance Revolution (DDR)”. The aforementioned game, DDR, is extremely popular with children and young adults. It involves moving on a small, portable dance floor while a video with instructions plays on the screen.
Research grants were dispersed by RWJF in order to study things like “the potential of physical activity video games to serve as innovative, cost-effective ways to help people recover motor skills after experiencing a stroke” or “health impacts of online mobile mini-games for people with type 2 diabetes.” Another group of 12 research grants will be awarded next year.
By-line: Heather Johnson is a regular commentator on the subject of CNA Classes Online. She welcomes your feedback and potential job inquiries at heatherjohnson2323 at gmail dot com.
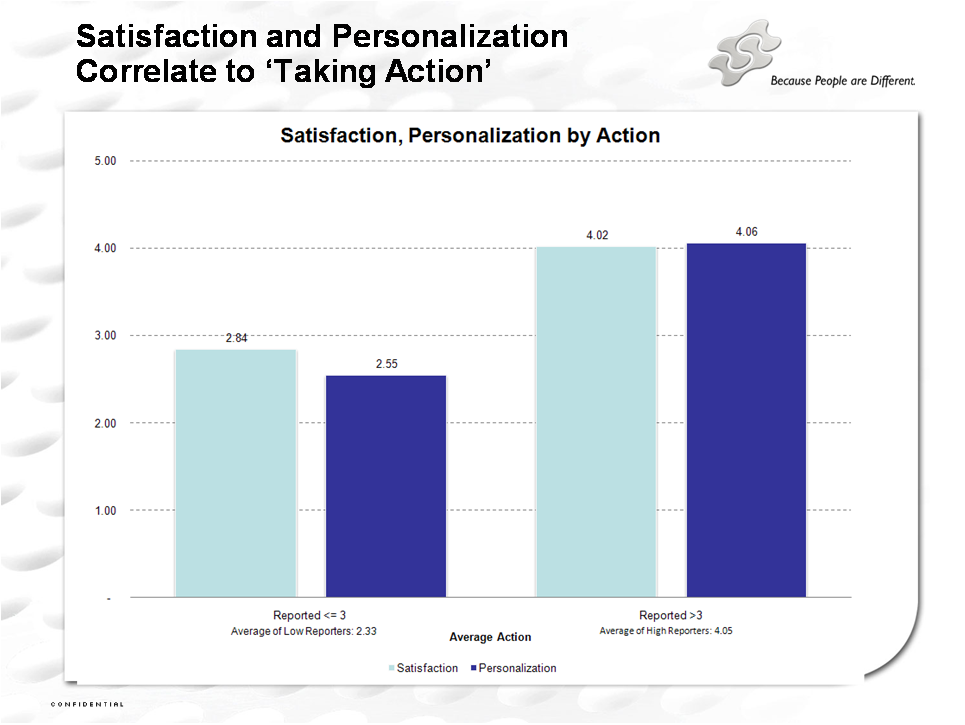
 I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.
I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.