On 12/4/07, USA Today had an article titled “Medicare cuts back on drugs covered by Part D” which talked about the fact that the average number of drugs covered by the 10 largest Medicare Part D providers shrunk by 26% from 2007 to 2008. Wow! At first glance that seems pretty dramatic compared to a commercial plan [whose shrinking coverage was not quoted].
It seems like most of the changes were driven by Medicare which the article says reduced the list of drugs it would reimburse including drugs pulled by the FDA, no longer being made, or were deemed “less than effective” by the FDA.
Tom Noland (Humana spokesman) said “As the Part D program develops, the size of the formulary is becoming more aligned with utilization patterns, consumer preferences, health outcomes, and value for consumers.”
The article also quoted a study saying that low-income enrollees in Texas were being switch to coverage that had 14% fewer drugs and 15% of all drugs offered requiring a prior authorization. [15% sounds very high to me.]
In the big picture, controlling costs by focusing on value is essential for our healthcare system to survive. Having an easy exception process [which doesn’t exist today] would allow that be tolerable by the general public. It will be an interesting debate on value at some point…how do you value different side effects (for example)?
On of my first healthcare projects back in graduate school looked at two different cancer treatments. One involved much more labor and had only moderate improvements in outcomes. The question of course was what to do with that – charge more for the one option, don’t do both, focus on outcomes, etc.
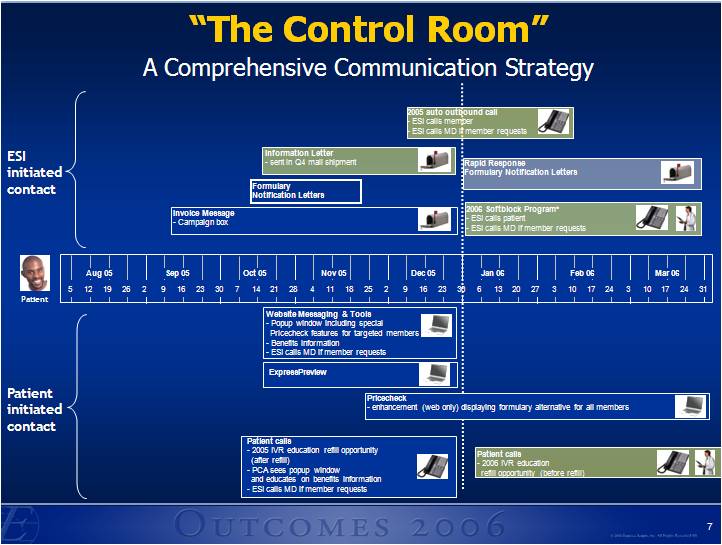
Back to Medicare…Hopefully, these companies have a good strategy for communicating and providing tools to these patients to ease the transition to the other drugs rather than wait for them to get rejected or see an unusually high copay at the counter when they don’t have time to get in touch with their physician without risking missing a day of therapy.

 January 15, 2008
January 15, 2008 





 He talks about the concentration of spending (based on Kaiser Permanente data):
He talks about the concentration of spending (based on Kaiser Permanente data):



