May 31, 2008
May 31, 2008 
On the positive side, there were no healthcare companies that “won” this “competition”. Winning being that you were rated as having poor customer service the highest percentage of times. (On the flipside, very few were included.) [full rankings here]
“We’ve seen a fall in customer service as we’ve gone into a recession,” said Richard D. Hanks, the president of Mindshare Technologies, a customer-service consulting company. “As the cost cutting occurs . . . they start to cut the wrong things.” (Article)

Not surprisingly, the people surveyed said that being knowledgeable, available, and friendly were very important. As we all know, the key attribute is knowledge and with the complexity of benefits, multiple systems that healthcare reps need to access, and turnover, this is a challenge.
It’s no wonder that everyone is trying to move people to self-service. In a related article, some of the benefits of self-service were clearly articulated:
“What better customer service is there than self-service?” ask the marketers. “It’s fast!” “It’s accurate!” “It’s convenient!” “It’s confidential!” (No more bystanders overhearing that triple-cheese, extra-mayo order.)
- People buy more. Customers spend 39% more per order at fast-food kiosks and are twice as likely to upsize than if a person takes their orders. (Machines are programmed to ask every time, and no one can overhear.) Customers also buy more at deli kiosks in supermarkets.
- More people buy. Good Web self-service allows for far more customers to be adequately served.
- People remain loyal. “You mean I’m going to have to upload all my data into a new bank? And learn a new system? No way.”
- People give the company high marks for customer service. Yes, funny but true. It’s hard to complain about a food order that you placed yourself, a transaction that you scripted or the way you pumped your own gas. When customer service is self-service, you have only yourself to blame.
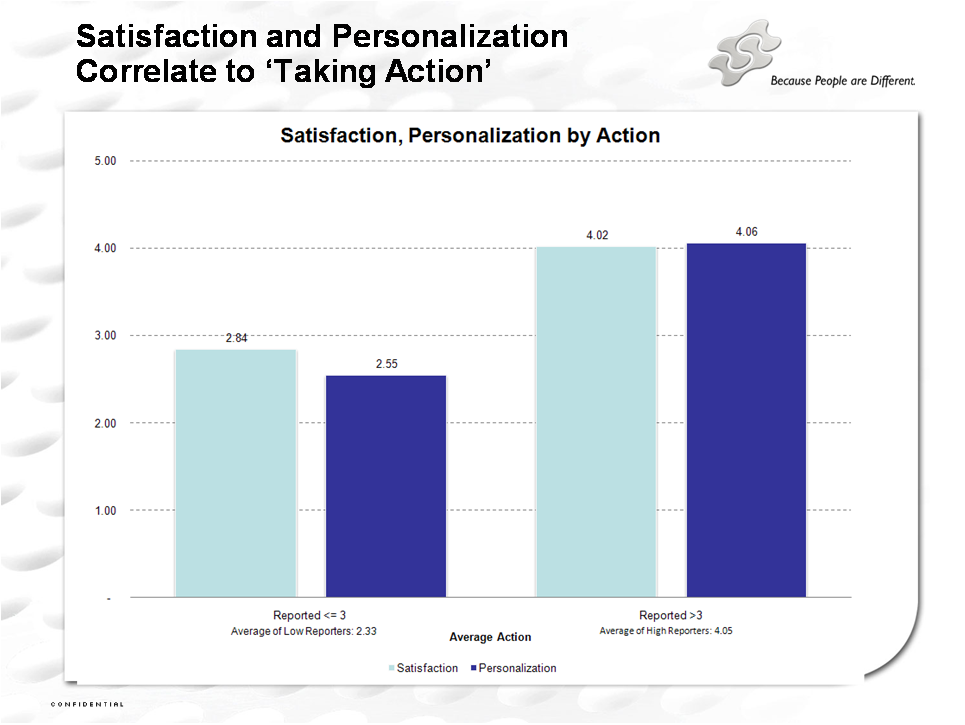
 I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.
I certainly think that more targeting is better although I might not always want you to tell me how much you know about me.