I am a big believer that we need to change our approach to how individuals manage their health. After a dinner with a financial planner friend of mine, it got me thinking what if we helped individuals plan for a long healthy life the same way we help them plan their careers or their finances. We have whole industries dedicated to helping people make smarter investment decisions for their retirement and job choices for their careers, but when it comes to our health we are rarely proactive.
According to Morgan Stanley, 90% of Americans think financial planning is important. Why? Three of the top reasons people undertake financial planning include:
- Making sure your money will last during retirement or rolling over a retirement plan
- Being prepared for a financial crisis such as a serious illness
- Caring for aging parents or a disabled child
The common thread through all of these reasons is personal health. Whether concerned directly about illness, both our own and that of our loved ones, or about our ability to enjoy our retirement to its fullest, personal health is a key component of a well-planned retirement.
The reality is life expectancy has increased dramatically. We may live 30 years in retirement. I would argue the quality of that retirement is even more dependent upon our health than our finances. Yet no one hires a “personal health coach” or creates a “personal health plan.”
It is about time we stop neglecting our future health. You can take control of your future health by developing a personal health plan. These simple steps can help you get started:
Step 1: Conduct a Personal Health Audit. Before you can build a plan you need to understand your base-line. You can’t map directions to your destination until you know where you are. When you meet with a financial planner the first thing they want to know is how much money you have saved for retirement. Your personal health plan is the same way. Do you suffer from any chronic illness? What is your height & weight? How much exercise to you get? What are your eating habits? Do you have any family history of disease? What type of pain do you suffer from? How is your mental health your relationship with your spouse and children? Capture everything and identify areas that need attention or improvement.
Step 2: Define Success. What does a healthy future look like? The second question a financial planner will ask you is how much monthly income will you need in retirement to live the lifestyle you want? The same is true for health. When do you plan on retiring? What hobbies do you have that you would like to pursue? Do you plan on having grandchildren? How will bad or good health impact all of these plans? Does your family history require you to focus on preventing cancer or heart disease or Alzheimer’s? The ability to visualize your health in the future both good health and your health if you let yourself go is a strong motivator for change. A point of note: Thinking about health 30 or 40 years into the future can be very abstract; I suggest breaking down your definition of success into annual targets is more manageable and motivating.
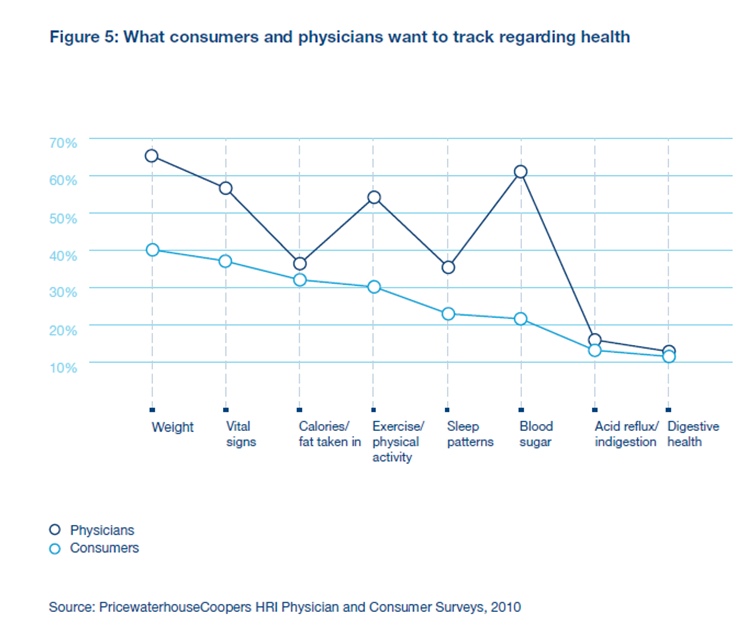
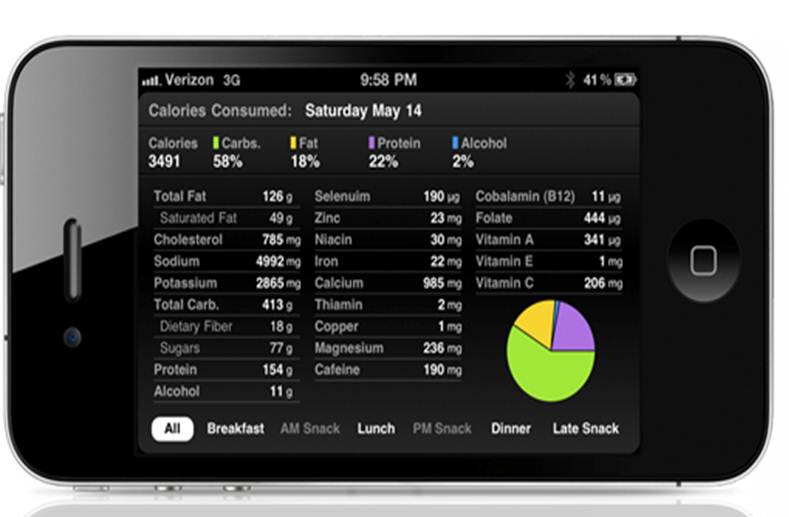
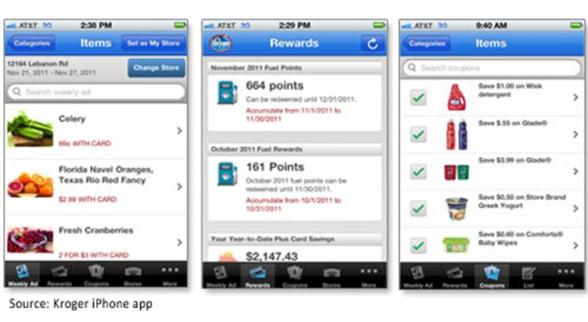
Step 3: Know your Personal Health Indicators of PHIs. By this point in the process you should have a sense of what measurements are most critical to your health. Develop a method for capturing your PHIs on a regularly basis. For some like weight you might update your PHI daily, weekly or monthly. For others like a PSA level for men at risk for prostate cancer, you might update it annually. I detail some of the more common PHIs here: http://www.billpaquin.com/do-you-know-your-phis/.
Step 4: Engage your Health Partners. Now that you have completed your audit, defined success and developed your most important PHIs it’s time for you to engage all of the people in your life who help you manage your health. This will include your family, your physician or other healthcare professionals; maybe you have a nutritionist, acupuncturist or other complimentary practitioner that you frequent. Inform them of your personal health plan and get their feedback and buy in. The more people who are on your side the greater the likelihood of success and the more people that know your health, the greater the likelihood you will have a plan that fits you and your goals.
Step 5: Build and implement your Plan. Building the right plan takes an understanding of what you learned in steps 1-4. By way of example, if you have a family history of colon cancer, you need to understand what behaviors help reduce your chances of getting this cancer, what preventative screening you should be getting and when you should be getting them. All of our plans should include a path to maintaining an ideal Body Mass Index that includes some form of daily exercise and nutrition plan, but we are all unique and will have plans specific to our health situations and desired goals. I do think it’s important to understand that no one is perfect 100% of the time, if you deviate from your plan for a day, week or even month, you are only one day from starting again.
Step 6: Review & Measure your progress. You can’t manage what you can’t measure. At some pre-planned interval you should step back and take stock of your progress. Use your annual physical or dental cleaning as a reminder to sit down and review your health plan. Personally I like to review different elements weekly or monthly, but find what works for you and stick with it. Like the stock market, it won’t be a straight line, but as long as the trend continues up over time you will be alright.
No one is responsible for your health but you. We all need to take a proactive approach to our health. Developing a personal health plan is a great way to insure you live a long, healthy and happy life.
About the Author
Bill Paquin is the Chief Executive Officer at Vertical Health, a publisher focused on improving patient care associated with back pain and endocrine disorders such as diabetes. He is a husband, father and writer who is passionate about and supports the creative destruction of our current healthcare system.

 January 1, 2013
January 1, 2013 





































{kind=link}