
 February 10, 2008
February 10, 2008 
I was looking for a book the other day to read on some of my flights and came across Health Care Communication Using Personality Type by Judy Allen and Susan A. Brock. I have just started reading it, but I related very well to their key assumptions:
- People prefer to communicate in different ways.
- Most people have a preferred style of communication.
- It is easier to communicate with some people than it is with others.
- A system exists which provides a simple framework for understanding these differences.
As I have mentioned before, I think that Myers-Briggs is a good framework for understanding people. I often pull up my notes about my personality type and can see that I respond as predicted to certain situations.
Applying some of their initial thoughts with my perspective, it would seem like there are some basic hypotheses that you could make in talking with patients.
- Extraversion: People that like to talk things out. Probably more likely to respond to verbal outreach.
- Intraversion: People that like to think things through. Probably more likely to respond to print (e.g., letter or web).
-
Sensing: People that like the specifics and the details. Probably more responsive to a detailed message (e.g., you can save exactly $X by doing this). Probably want to see the path of exactly who needs to do what.
-
Intuition: People that see the big picture. Probably more responsive to a communication that helps them understand the impact of their decision on overall healthcare trend. Probably want to understand their options versus being guided down a path.
-
Thinking: People who are very logical. They should respond well to automation and would want an if/then type of message.
-
Feeling: People that are more emotional. They would likely respond best to live agents where they could empathize with them and potentially even respond to a “peer pressure” type of message (e.g., most people are now using generic prescription drugs).
-
Judging: People that are organized, punctual, and focused on getting things done. They would likely respond to messages about how to save time and money delivered in the quickest format possible.
-
Perceiving: People that are flexible, don’t plan ahead, and are often more disorganized. They would likely respond to a just-in-time message, a compliance reminder, and a communication process that did everything for them (e.g., you should go in for a colonoscopy…would you like us to schedule that for you).
Obviously, one framework doesn’t solve everything, but I expect that there is a lot more to gain from this book as I read through it. I was just so excited after the first section given my interests that I wanted to post this quick entry.



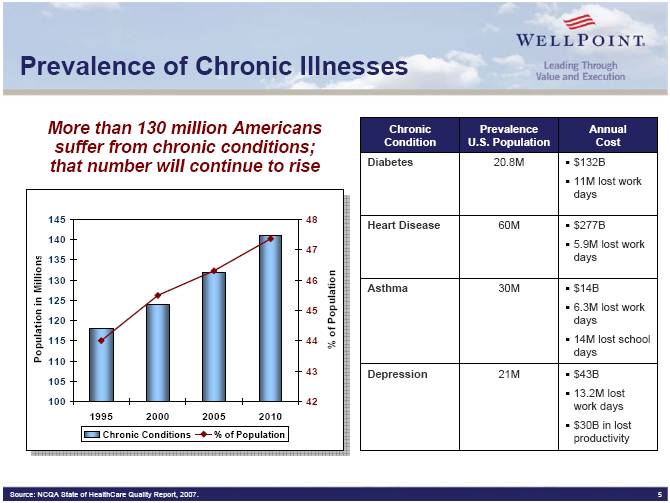


 He talks about the concentration of spending (based on Kaiser Permanente data):
He talks about the concentration of spending (based on Kaiser Permanente data):



