
 April 15, 2008
April 15, 2008 
If you ever needed proof that communications matter, here are a few recent examples:
1 – Look at all the “flap” that Obama is taking over the use of the word bitter. It may cost him the nomination.
2 – In another example, look at Colbert on Larry King Live last night (go to 5:20 on this YouTube video) where he talks about Obama passing around his “Hope Bong” to the young people of America.
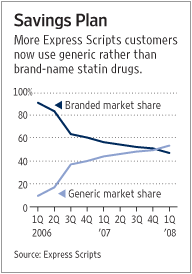
3 – And back in healthcare, Express Scripts finally announced their Center for Cost-Effective Consumerism in the WSJ today.
“Express Scripts’ experiment with incentives is rooted in a discipline called behavioral economics, which draws heavily from principles of social and cognitive psychology. The field attempts to understand why people make economic decisions that aren’t based solely on saving or making money.”
I have talked about this HMG (or cholesteral lowering drugs) program before on the blog, but they have some results revealed in the article. The article goes on to talk about the research done and some of the findings:
“So Express Scripts surveyed thousands of customers to understand better their concerns about generics. It learned some were uncomfortable with how to tell their doctors they wanted to switch, or felt it wasn’t their role as patients to bring up the topic. Others found the whole topic too complicated to bother with.
With those concerns in mind, Express Scripts made several changes to how customers were informed about simvastatin, such as shortening the text in its literature and changing its color and including a letter that patients could just hand to their doctor requesting a switch.
The company also framed the message to focus not merely on cost savings, but on how generics can be the better value — explaining that drugs that cost more but don’t do more aren’t a better value. People often believe branded or costlier drugs simply are better, says Dr. Nease, whereas Express Scripts’ new message stated that the “best buys” are drugs that cost less and do the same thing.”
 This is important. Driving personalization through multi-modal messaging that helps simply complex messages into digestible information that links the constituents in healthcare isn’t easy.
This is important. Driving personalization through multi-modal messaging that helps simply complex messages into digestible information that links the constituents in healthcare isn’t easy.
As the article points out, Medco and Caremark are going down similar paths as are many of the managed care plans. Communications is becoming the key area of differentiation in healthcare as it has been in other industries for years.











{kind=link}