August 22, 2014
August 22, 2014 
I think many of are familiar with Google’s use of the term “Moon Shots” and to a lesser degree their Google X projects. I was inspired to see who in healthcare is using the term and think about a few moon shot ideas myself.
- MD Anderson is one company that talks about moon shots in terms of curing cancer.
- Google has their moon shot around the human body and their Calico project.
I didn’t find much else out there (although I’m sure there is).
So, here’s some of my thoughts:
- Curing cancer. But I think this is one many people think about.
- Creating a healthcare system that people actually understand. That would be great!
- Making healthcare a positive experience. Not easy, but it should be achievable in many settings.
- Preventing disease progression. Maybe too simple, but there has to be some stretch about using data to predict risk and trigger proactive, personalized engagements that successfully change behavior.
- Integrated data. The idea of interoperability of data across the care continuum with the ability to make it actionable would be great.
- Remote monitoring of people without them having to do anything. The Internet of Things will make this much easier (some day), but the idea of simply integrating technology into our lives to monitor us and look for ways to improve our life is a great goal.
- Integrated devices such that our decisions are improved would be great. A device that knows I’m getting hungry and that I’m about to pass a McDonalds could suggest a healthy alternative.
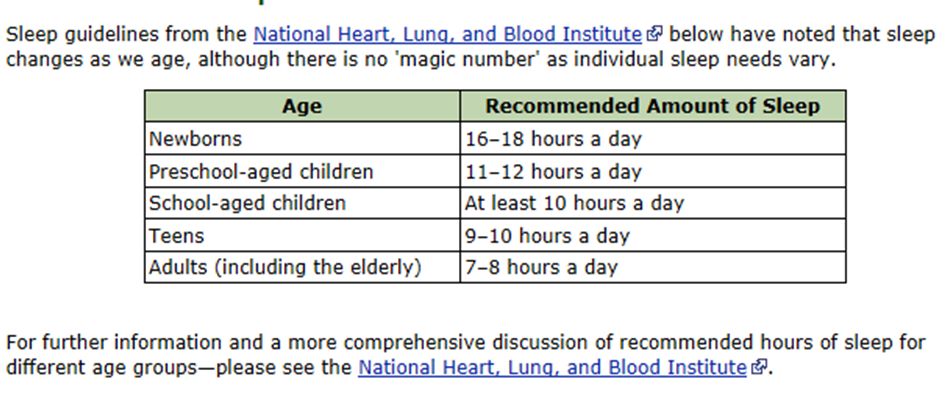
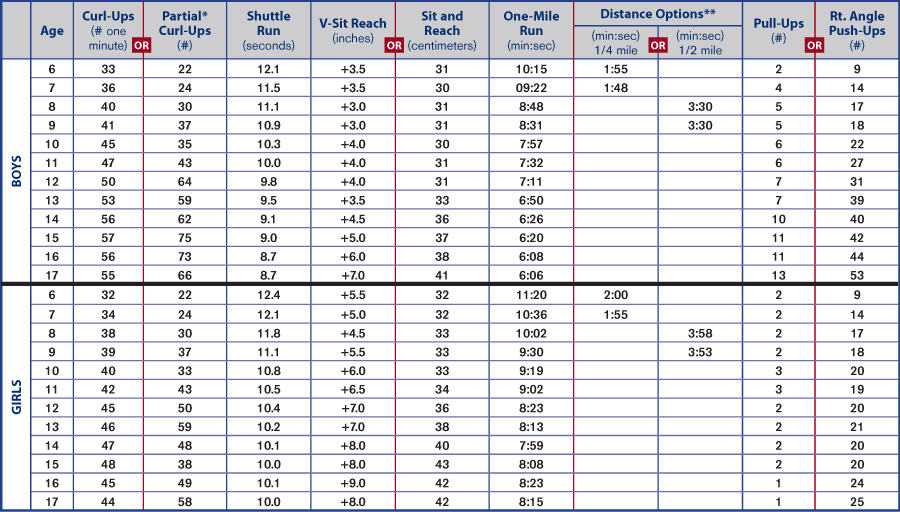
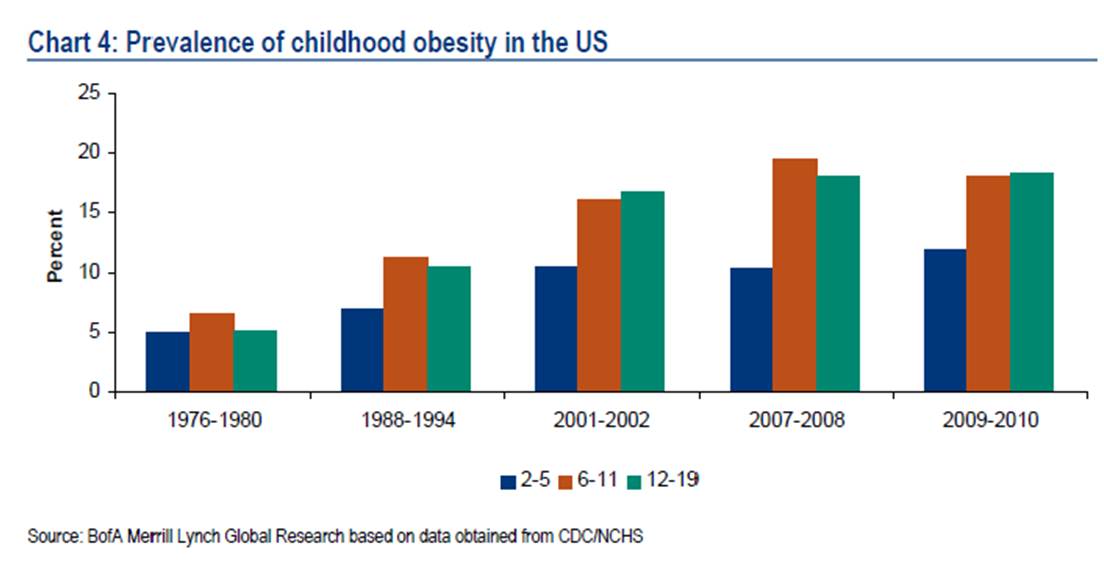
- Reducing global obesity by teaching kids about health. This is a great one with complexity like addressing food deserts, sleep patterns, food selection, and general attitudes about health.
- Eliminating negative stress in order to improve health. This is another tricky one as our lives become more and more stressful.
I’ll leave the list open…what would you add? I know there are some big stretch thinkers out there.
- Digital pills you can print in a 3D printer
- “Doc in a box” solutions that could be in every home where the physician can get your vitals and interact with you all virtually.
- Self-healing band-aids that turn into skin.
- A pill that you take once a year, and it doses you ever day.
- A machine that can actually diagnose you (like that mirror in the one cholesterol advertisement).
- A pill to cure addition to cigarettes and other addictive substances.
- Food that turns bad cholesterol into good cholesterol.