January 4, 2008
January 4, 2008 
I found this great list of factoids or Did You Know statements at PharmacySatisfaction.com. Here were some of my favorites or more interesting ones.
- The biggest reason for not taking all medications as directed was simply, “I forgot.”
- The number one concern across all pharmacy users is that their prescriptions are filled accurately.
- The most useful feature those Web sites offer to them, the survey found, is the ability to order refills online.
- Nearly three in 10 order their refills online.
- Customers average three visits each month to their pharmacy.
- Only about 1-in-5 pharmacy customers, overall, say that they use a loyalty card that provides points, discounts or other savings.
- While the majority of loyalty card users are satisfied with the expected cost savings by using their card and with the ease of enrolling and understanding the benefits of their card, fewer than 1-in-4 card users are highly satisfied.
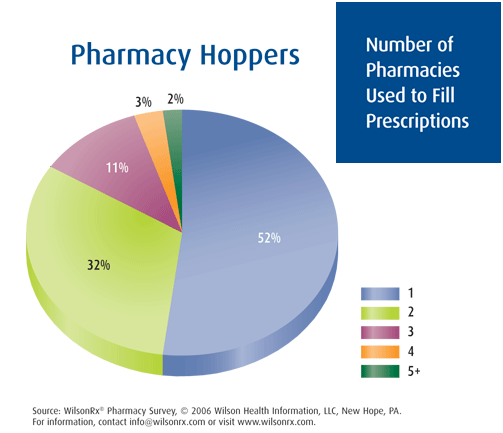
- The drug store industry remains largely up for grabs, with nearly half of pharmacy customers saying they use more than one pharmacy to fill prescriptions.
- Pharmacy use varies considerably by population. Chain pharmacies are most commonly used among residents of areas with more than 100,000 people. Independent pharmacies are most commonly used among rural respondents (areas with less than 100,000 people). Use of independent and mass merchant pharmacies decreases as population increases. Chain, food store, mail/online, and clinic pharmacy use tend to increase with population.
- However, as pharmacy customers age, they are much less likely to use chains and considerably more likely to use mail/online and clinic pharmacies.
- Seven-out-of-ten pharmacy customers indicate that they “definitely would” or “probably would” use their local pharmacy if they could receive the same amount of medication at the same price as their mail-order pharmacy.
- The heaviest users of prescriptions are survey respondents in their 60s, averaging 5.4 new scripts and 29.2 refills per year.
- How long patients have to wait for their scripts to be filled is a key component of customer satisfaction.
- The average survey respondent is spending a considerable sum each month on drugs at their pharmacy—$82 on average (versus $57 a month on food and groceries at their pharmacy).
- An average of 85.9% of computer owners/users use the computer to improve their health by looking for information about diseases.
- Much has been written about the value of closer pharmacist-patient relationships, but Americans seem to feel far more connected to their physicians, dentists and nurses than to their pharmacists. That’s clearly not all pharmacy’s fault; the same survey respondents agreed that they were usually given the opportunity to speak with their pharmacist when filling their last prescription. What’s more, pharmacists ranked a close second to doctors as sources of information about medications.
- Walgreens’ “Dial-a-Pharmacist” initiative, launched in February 2006, allows non-English speaking patients to connect with pharmacists speaking 14 different languages.
- Independent pharmacy customers have the most trust in pharmacists, while mail/online customers have the least. Compared to last year, customers of all types of pharmacies place more trust in their pharmacist as a source of information.
- More than one-third of pharmacy customers failed to fill all their prescriptions last year, and only 35 percent of all respondents said they were fully compliant on the medications they did take. Nevertheless, refill reminders from the pharmacy remain relatively rare, most patients profess.
- In general, older patients tend to be more compliant than their younger counterparts.
I mentioned poly-pharmacy a few days ago, but here is some data about how many pharmacies patients use.
 He talks about the concentration of spending (based on Kaiser Permanente data):
He talks about the concentration of spending (based on Kaiser Permanente data): use that to compel the legislators to act but doesn’t it seem strange to have an end customer comment about the supply chain relationship of two entities. What am I talking about?
use that to compel the legislators to act but doesn’t it seem strange to have an end customer comment about the supply chain relationship of two entities. What am I talking about? some family objectives, a financial planning objective, and a few personal objectives (e.g., run a 1:40 half-marathon).
some family objectives, a financial planning objective, and a few personal objectives (e.g., run a 1:40 half-marathon).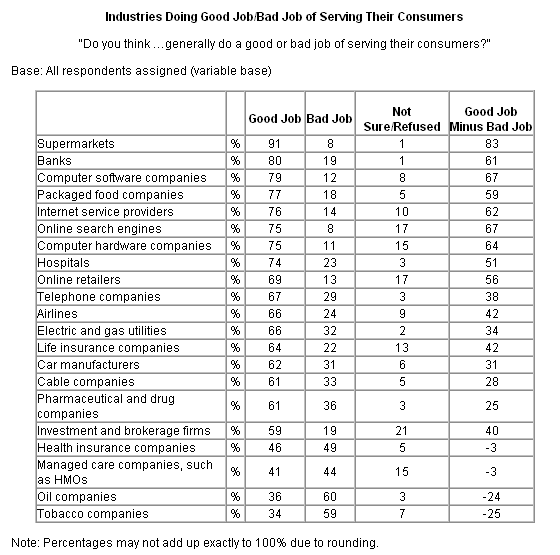
 I have a group of guys who I play poker with at least once a month. We play
I have a group of guys who I play poker with at least once a month. We play 
 Getting back to the article…He offers several good examples of sticky messages which are primarily what I would call rallying calls for organizations. In healthcare, the key is to find these simple messages that compel people to act. So, bottom lining it, he gives six basic traits:
Getting back to the article…He offers several good examples of sticky messages which are primarily what I would call rallying calls for organizations. In healthcare, the key is to find these simple messages that compel people to act. So, bottom lining it, he gives six basic traits:
 I don’t know the answer here, but I am sure someone out there does. The question is whether healthcare professionals are bigger utilizers of healthcare services (e.g., MRIs, prescriptions, well visits, etc.). I always want to know that from service providers. If you are selling me a CRM (
I don’t know the answer here, but I am sure someone out there does. The question is whether healthcare professionals are bigger utilizers of healthcare services (e.g., MRIs, prescriptions, well visits, etc.). I always want to know that from service providers. If you are selling me a CRM ( In
In