I must admit when I saw there was controversy over the content for the premier of the new show Eli Stone that I was really surprised. My view was that it was a show with an interesting story line not a news report. I honestly didn’t realize that the topic of vaccines causing autism was a real topic. (Maybe I just haven’t paid attention.)
I saw several blog entries about it:
I think the quote from another About.com section sums it up pretty well from what I have read:
“I personally believe that the vast majority of people involved in this debate are telling the truth as they see it. But those truths are in direct conflict with one another. That’s where the writers of Eli Stone got it right: today, in the autism community, we are living through what feels almost like an epic battle. Whose truth is truer? Until some as-yet-undefined event provides absolute certainty one way or another, people will continue to take sides based on their beliefs and on the evidence – valid or not – of their own eyes.”
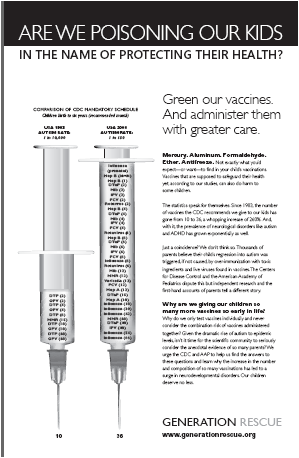
I am clearly not a clinician and haven’t done the research on this topic, but I find it interesting. I likely would have let it slip by me except when I picked up the USA Today on Tuesday I saw a full-page advertisement titled “Are we poisoning our kids in the name of protecting their health?”. It caught my attention so kudos to the designer. So, I read the advertisement and went to the website for Generation Rescue to learn more.
“We surveyed over 9,000 boys in California and Oregon and found that vaccinated boys had a 155% greater chance of having a neurological disorder like ADHD or autism than unvaccinated boys.” [see their study details here]
From the advertisement, it points out that the autism rate in the US in 1883 was 1 in 10,000 and in 2008 is 1 in 150. That is pretty scary. When I was a kid, I don’t remember knowing kids with autism or ADD/ADHD or peanut allergies or lots of other conditions. Today, I know and have friends with kids with each of these conditions. It certainly is more prevalent (or more diagnosed).
The point of the advertisement is that we have increased the number of vaccines we give our kids from 10 to 36 since 1983 and that the over-immunization with toxic ingredients (mercury, aluminum, formaldehyde, ether, antifreeze) and the live viruses have caused this. Of course, the Centers for Disease Control (CDC) and the American Academy of Pediatrics dispute this. I don’t know the answer, but I know that it’s not easily going to get resolved and no magic trial like the show is going to resolve it. It’s not different than many issues in healthcare where there isn’t great comparative data and things are not black and white.
Anyways, watch the show. It’s good. On what the right answer is. I don’t know.


 February 29, 2008
February 29, 2008