
 December 28, 2007
December 28, 2007 
I understand the logic if I am the pharmacies of reaching out to the patients to motivate them and  use that to compel the legislators to act but doesn’t it seem strange to have an end customer comment about the supply chain relationship of two entities. What am I talking about?
use that to compel the legislators to act but doesn’t it seem strange to have an end customer comment about the supply chain relationship of two entities. What am I talking about?
The Coalition for Community Pharmacy Action which is made up of the National Community Pharmacists Association (NCPA) and the National Association of Chain Drug Stores (NACDS) conducted a survey of 1,000 pharmacy patients about the slow reimbursement of Medicare Part D drugs by the PBMs and upcoming cuts in Medicaid reimbursement. Not that I don’t think it’s an issue, but I find it hard to believe consumers knew about the issue and weren’t “coached” into answers based simply on the way the questions were asked. Regardless, the results were:
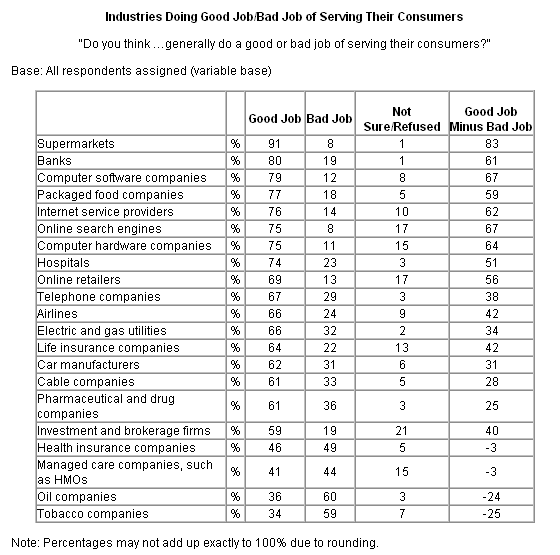
- 83% said that it was unfair that “PBMs and prescription drug plans keep money as long as possible, allowing them to earn interest on it, while pharmacies must continue to provide their services and prescription drugs upfront to patient even though they haven’t been paid.” [Do you think the average patient would say that if you simply asked them what they thought about reimbursement policies for pharmacies?]
The survey is obviously to drive support for two bills – H.R.1474, the Fair and Speedy Treatment of Medicare Prescription Drug Act of 2007, and S.1954, the Pharmacy Access Improvement Act (PhAIM) of 2007 which require complete and accurate Part D claims submitted electronically be paid within 14 days by electronic funds transfer, and paper claims within 30 days.
- 78% thought it was unfair that “under the new rule, pharmacies that participate in the Medicaid program would have to sell generic drugs at a loss.” [I believe it’s possible, but I would like to see the math here. Is it net of their costs? Are their costs direct labor or is it a volume issue?]
“We have reached critical mass in our efforts to rectify the debilitating consequences of the Medicare Part D and Medicaid reimbursement systems,” said Bruce Roberts, RPh, NCPA executive vice president and CEO. “The sentiments expressed by community pharmacies, members of Congress, and organizations such as NCPA and the National Rural Health Association are well known. The missing voice has been the patients who are adversely affected by the consequence of community pharmacies being squeezed to the breaking point. Now we have a comprehensive scientific survey indicating patients find the reimbursement policies objectionable and are supportive of the pending legislative solutions that should spur action in the halls of Congress.”
I am a big believer in the independent pharmacy. They have and continue to play a vital role in many communities and serving patients in a very hands-on way. As the market has changed, it has been difficult. Seniors, who I believe are disproportionately represented at the independent pharmacies, were cash paying customers for a long time. Medicare Part D changed that and took away a great source of cash flow and margin.

 some family objectives, a financial planning objective, and a few personal objectives (e.g., run a 1:40 half-marathon).
some family objectives, a financial planning objective, and a few personal objectives (e.g., run a 1:40 half-marathon).
 I have a group of guys who I play poker with at least once a month. We play
I have a group of guys who I play poker with at least once a month. We play 
 Getting back to the article…He offers several good examples of sticky messages which are primarily what I would call rallying calls for organizations. In healthcare, the key is to find these simple messages that compel people to act. So, bottom lining it, he gives six basic traits:
Getting back to the article…He offers several good examples of sticky messages which are primarily what I would call rallying calls for organizations. In healthcare, the key is to find these simple messages that compel people to act. So, bottom lining it, he gives six basic traits: [By the way, as I have previously disclosed, I own no ESRX stock or other stocks individually. I only invest in mutual funds…and do very well with it.]
[By the way, as I have previously disclosed, I own no ESRX stock or other stocks individually. I only invest in mutual funds…and do very well with it.]
 I don’t know the answer here, but I am sure someone out there does. The question is whether healthcare professionals are bigger utilizers of healthcare services (e.g., MRIs, prescriptions, well visits, etc.). I always want to know that from service providers. If you are selling me a CRM (
I don’t know the answer here, but I am sure someone out there does. The question is whether healthcare professionals are bigger utilizers of healthcare services (e.g., MRIs, prescriptions, well visits, etc.). I always want to know that from service providers. If you are selling me a CRM ( In
In 








{kind=link}
{kind=link}