
I found this site listing some of the top diabetic bloggers and also found this infographic there.
http://www.sharecare.com/static/sharecare-now-diabetes

 November 13, 2012
November 13, 2012  0 Comments
0 Comments
I found this site listing some of the top diabetic bloggers and also found this infographic there.
http://www.sharecare.com/static/sharecare-now-diabetes
November 13, 2012 0 Comments
A physician asked me this a few months ago, and I thought it was a great point. We were discussing the fact that there are often times when we (the medical institution) may try too hard to “cure cancer” (see some of the points in my post about palliative care). When it’s viewed as a war that has to be won, it may be that too much effort is spent to beat cancer into remission rather than thinking about the patient’s experience. (see cartoon from naturalnews.com below)

A friend game me this example…While his brother’s cancer was in remission, the toll of the chemo and the other treatments was so much that he was never able to work again. The patient would have preferred to be able to work a few more years and die of cancer, but that discussion never happened.
In general, I believe most physicians would consider this a failure. They’re taught to “beat” the disease not to back off and let the disease “win”. But, I often hear about the “war on cancer“.
Even after 40 years, we still have a large amount of annual deaths from cancer.

November 12, 2012 0 Comments
Unfortunately, I don’t think a lot of this will surprise many of you, but it’s scary to think about the impact of obesity across different industries. For some of them this is big business. And, while I don’t think employers have fully realized how to focus on this from a “wellness” or “disease management” perspective, I think that will change.

November 12, 2012 0 Comments
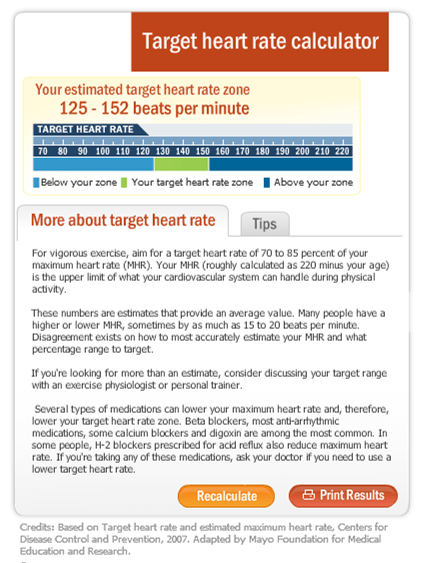
If you’re like me, you get on the treadmill or other exercise equipment at the gym and see it talk about exercising at X% of your maximum heart rate. Or, you get a heart rate reading on the device and wonder what it means.
It appears that the simple answer is to take 220 minus your age. For example, if you’re 30, then your maximum heart rate would be 90.
Now, when I plugged my age into a Mayo Clinic site, it shows me all the caveats about this answer.
November 7, 2012 0 Comments
Specialty drugs are expected to represent 40% of total Rx spend by 2020 so guess what…they’re the focus. Generic Rxs represent 80% of the oral drugs dispensed today and are low cost. PBMs, pharmacies, and payors are and should be focusing on specialty drugs.
Of course, this is driving a shift towards price compression and medical management types of functions like PA, UM, ST, case management, and even disease management.

So…what should your specialty pharmacy be focused on?
I think this is going to require a tighter coupling of population health companies with specialty pharmacies and potentially better leveraging pharma manufacturers as partners versus suppliers.
This is not just a cost challenge…this is about outcomes. I usually think of it in terms of “The Triple Aim” which is about cost, quality, and experience.
If you look at your specialty pharmacy partner, I think you could put them in 3 buckets:
November 7, 2012 1 Comment
I got to see Dan Buettner, author of BlueZones, present a few times and love some of the insights from his research. The other day, there was a list of these nine lessons in USA Today:
It’s worth digging into his research if you’re looking at how to live longer.
November 7, 2012 0 Comments
I’m getting a little backed up in terms of articles and ideas that caught my eye so I’m going to share a few of them here.
November 6, 2012 0 Comments
While I do applaud the creative concept here, I wasn’t overly impressed with the creative itself. At the end of the day, the question for me is results. Did it pay for itself? Did it get more people to get colonoscopies (in the target audience) than otherwise would have? I’m unsure of that.
Here’s what I did find in a HealthLeaders article…At the end of the day, I’d want to compare that to a program we did at my last company for UHG in this area.
The campaign also netted 44 colonoscopy appointments. Of those 44 appointments, 13 were current Good Samaritan patients and 31 were new to the hospital. Forty-three of the 44 scheduled an appointment through the call center and one booked online. Of those who called, 27 cited the radio spot as how they found out about the service. More than half of the patients were in the target group of 50–59 year olds, with 24 female and 20 male.
November 5, 2012 2 Comments
Healthcare in 2020 by Steve Jacob is a great book. Lots of facts. Lots of relevant information. A quick read. Well referenced. If I could, I would send this to every client I’ve ever worked with to help them understand why changing healthcare is so important.
I’m going to share a handful of things from the book here. Even if I could provide you with a detailed summary, I wouldn’t. You need to read this book.
Some scary data points. This book was a great reinforcement of some of the projects I’ve been involved with trying to accomplish the Triple Aim – Quality, Cost, Experience.
November 2, 2012 0 Comments
I came across the chart below and thought I would post it with my perspective on trends for next year.

November 2, 2012 0 Comments
 This seems like an interesting question, but one with perhaps a straightforward answer. With NY and NJ devastated by Superstorm Sandy and almost 4M still without power, should NY try to hold their marathon this weekend? Seems like a clear no to me.
This seems like an interesting question, but one with perhaps a straightforward answer. With NY and NJ devastated by Superstorm Sandy and almost 4M still without power, should NY try to hold their marathon this weekend? Seems like a clear no to me.
I do understand the fact that this is a big revenue event for the city. I do understand that you want to show your ability to recover from the storm. BUT, it takes resources – volunteers, police, hotels, food, and other efforts to pull this off. Wouldn’t those resources be better focused on the people that are still trying to dig out of their homes and get power?
November 1, 2012 0 Comments
The same Wired article had some highlights from their Wired Health Survey. Here’s a few data points that caught my attention:
November 1, 2012 0 Comments
I was reading Wired Magazine (Oct 2012) last night, and I came across this article “Living By Numbers: The Wired Guide To Health”. It gives “18 data-driven ways to be happier, healthier, and even a little smarter.” In my words, it’s a nice cheat sheet of some basic things we should all know (and many of which I’ve blogged about over the years).
October 29, 2012 0 Comments
I’m not sure whether to call it a movement or a trend or some other term, but I think it’s very interesting. This idea of capturing and tracking data manually and through devices fits very well with the idea of “Know Your Numbers” in healthcare.
Here’s the descriptionof Quantified Self from Wikipedia:
The Quantified Self is a movement to incorporate technology into data acquisition on aspects of a person’s daily life in terms of inputs (e.g. food consumed, quality of surrounding air), states (e.g. mood, arousal, blood oxygen levels), and performance (mental and physical).
The movement was started by Wired Magazine editors Gary Wolf and Kevin Kelly in 2007as “a collaboration of users and tool makers who share[d] an interest in self knowledge through self-tracking”. In 2010, Wolf spoke about the movement at TED, and in May 2011 the first international conference was held in Mountain View, California.
Quantified Self is also known as self-tracking, body data and life-hacking. It is described in articles such as this one in the Economist and this in Forbes.
With an increasing amount of devices on the market that can be integrated (e.g, FitBit), we will see a huge rise in remote patient monitoring where the patient takes a greater role in this effort. Even know you are seeing more efforts to integrate devices into the “smart home” with a focus on older patients, but I think this smart home concept will continue to grow.
This Slideshare presentation is a nice summary…
October 27, 2012 0 Comments

Source: Mount Sinai Medical Center
October 25, 2012 0 Comments
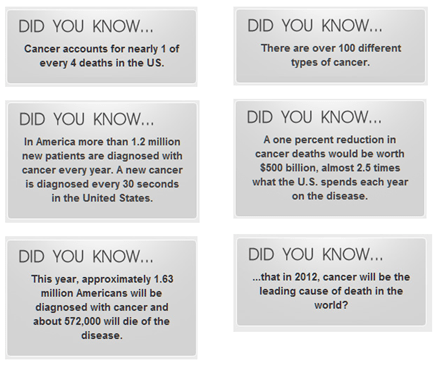
If you were like me, you were surprised and impressed to see all the Stand Up To Cancer signs at last night’s World Series game in San Francisco. It was impressive, but it made me wonder who this company was. Here’s some text from one of their press releases.
Stand Up To Cancer (SU2C) — a program of the Entertainment Industry Foundation (EIF), a 501(c)3 charitable organization — raises funds to hasten the pace of groundbreaking translational research that can get new therapies to patients quickly and save lives. In the fall of 2007, a group of women whose lives have all been affected by cancer in profound ways began working together to marshal the resources of the media and entertainment industries in the fight against this disease.
SU2C’s “Dream Team” approach to funding translational cancer research enables scientists from different disciplines at research centers across the country and internationally to collaborate on projects geared toward getting new, less toxic treatments to patients as quickly as possible. Monies also support innovative cancer research projects that are often deemed “too risky” by conventional funding sources. Sixty-five institutions are currently involved. As SU2C’s scientific collaborator, the American Association for Cancer Research, led by a prestigious SU2C Scientific Advisory Committee, provides scientific oversight, expert review of the research projects and grants administration.
I also grabbed a screenshot of some of the factoids from their website:
October 25, 2012 0 Comments
Whenever you go to the pharmacy, they always ask you if you have questions and make you sign off that you were offered counseling. It begs the question of whether anyone actually does. I just got this survey data e-mailed to me, and I wanted to share it since it was surprising to me and from RxAlly.
I also found it surprising that people don’t think their pharmacist can help them make healthcare decisions. This is certainly relevant in the Medicare world where AARP and others have partnered with pharmacists traditionally. Additionally, I think it limits some of the longer term opportunities for pharmacy, pharmacists, and PBMs. I’ve always thought that given their frequency of patient intervention that there would be lots of opportunities to leverage the pharmacist at the POS to close care gaps and be very engaged in the overall care and driving health outcomes.
Only 15 percent of U.S. adults have ever discussed a medication maintenance regimen with a pharmacist and only 49 percent have discussed any new medication with a pharmacist. Less than 20 percent (18%) of U.S. adults trust a pharmacist most to help guide and inform healthcare decisions for themselves and their families. A majority of people trust their doctor most (72%), followed by friends and family (36%), spouses or significant others (36%) and the internet (22%).
Source: RxAlly
http://rxally.com/rxally-news.html
October 23, 2012 0 Comments
The ideas around Population Health are certainly critical both to us as a country to eliminate the waste in our healthcare system, but they are also foundational in a move from a fee-for-service (FFS) environment to an outcomes-based payment model. Interesting, if you look at a study that was just released, it continues to show a disconnect within the provider community. (Study is Population Health Management In Physician Practice: A Call To Action.)
I believe some of this stems from the costs associated with the build out, integration, and use of these technologies in today’s environment. But, I think some of this stems from a broken connection between national policy, localized implementation, and payer coordination around key healthcare issues such as obesity.
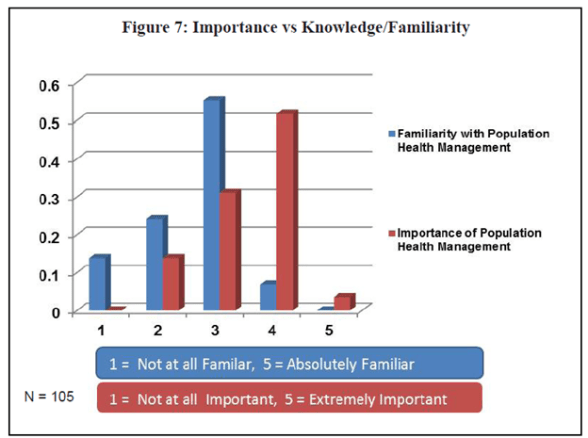
The following paragraph from the same document is also very telling.
“With 72% of respondents reporting that they had either already adopted or were in the process of adoption a patient-centered model of care, it was interesting that only 19% of practices self-reported as Patient-Centered Medical Home (PCMH) and only 10% as an Accountable Care Organization (ACO). Considering the critical role that population health management will play in both types of practice models, the data suggest that while they are undertaking population health management initiatives, many practices may not yet be at a level of transformation to warrant presenting as PCMH or ACO at this point in time. Also interesting is that of the 11 practices that did self-report as ACO, only 5 of the 11 also reported as PCMH – showing again perhaps another disconnect or struggle with implementation and understanding. PCMH, after all, has been described as “foundational” to Accountable Care Organizations.”
A lot of this change won’t be done by physicians, but it was promising to hear in the same report that:
So, how are those resources being used today? And, how do these resources get integrated into an overall care strategy for the patient? Are notes shared with external care managers? How do we find the right point person? How does an external payer team for MM coordinator with the local resources for something like discharge planning?
October 23, 2012 1 Comment
This is one of those terms that is thrown around a lot just like Medical Management or Disease Management.
I thought it would be helpful to define the 3.
Population Health Management (PHM) is…
“Programs targeted to a defined population that use a variety of individual, organizational, and societal interventions to improve health outcomes” (Mathematica Policy Research Issue Brief, August 2011)
Medical Management (MM) is…
“The general term often applied to the practices of utilization management (UM), case management (CM), and disease management (DM), alone or in combination with each other.” (Trends and Practices in Medical Management: 2001 Industry Profile)
Disease Management (DM) is…
“An approach to healthcare that teaches patients how to manage a chronic disease.” (Disease Management on About.com)
Is that clear as mud?
In today’s world, everything is patient-centric so that doesn’t differ between the three. Obviously, DM is a part of MM, but I rarely hear people talk about MM as a part of PHM which it seems to be to me. But, I don’t think of most MM type programs taking on the macro level change that PHM implies to me. PHM implies things like public health or broad programs like BlueZones. It implies looking at things like plan design, incentives, social trends, workplace culture, and other aspects of change that are necessary to create change and sustain change.
Here’s the Care Continuum Alliance’s full description of PHM (or as they call it here – population health improvement):
Key components of the population health improvement model include:
The population health improvement model:
And, if you read articles about PHM, these macro issues don’t seem to be the focus. The focus seems to be mostly on the technology to accomplish PHM. There are obvious challenges and key success factors there. (Recent commentary on PHM.)
October 16, 2012 0 Comments
Medicare offers people free preventative care which includes a variety of things:
(This list is from http://www.medicare.gov/coverage/preventive-and-screening-services.html.)
Now, while HHS says that over 32M people used these services in 2011, this is only 66% of Medicare beneficiaries. This varies by state with 48.1% of people in Wyoming taking advantage of this benefit while 71.1% of people in Delaware take advantage of the benefit.
I’m not sure of the root cause, but I suspect a lot of it has to do with education. Beneficiaries don’t understand what’s free. They don’t understand how to take advantage of the benefit, and physicians aren’t reinforcing this.
October 16, 2012 1 Comment
I was just watching the Verizon advertisement where they show data in a few ways. While their charts are all basically the same, it made me think about different ways of representing the same data. We all know that this is an important thing as we evaluate the effectiveness of different programs.
Let me highlight four different ways of representing two data elements. In this case, I’m comparing two programs. The first program (A) had a yield of 20% and the second program (B) had a yield of 23%.
I could show the data in two different charts where I simply change the y-axis.

October 15, 2012 0 Comments
This video is a little slower going than I had imagined, but it makes a series of tough points about the soda industry and its impact on our healthcare. See http://therealbears.org for more information.
October 11, 2012 0 Comments
I love where the future of healthcare technology is going. If you missed the Health 2.0 Conference this week, you can see a lot of the presentations now online for FREE! It’s very cool.
At the same time, I think this infographic from the Institute of Medicine reinforces some of the key points.

October 10, 2012 0 Comments
We should all know this, but not many of us do it.

October 10, 2012 0 Comments
I saw a mention of WellnessRx from Health 2.0 and went to look at them. I found this infographic which I think is interesting and reinforcing of the value of biometrics in population health management.

October 10, 2012 0 Comments

I keep seeing buzz about the Big Bird comment about PBS from the Presidential Debate from last week. As always, I interpret things differently. To me, this shows Romney’s willingness to make tough and perhaps unpopular decisions (like raising taxes for the Middle Class). At some point, these things may be critical.
Sure…the PBS budget may be small, but at some point, we as a country need to focus on how we cut costs to reduce our deficit. (See US debt clock.)

This reminds me a lot of the discussions we used to have to have as a PBM with employers or labor unions about their benefits. It goes back to the basic framework of “you can’t have your cake and eat it too”. Everyone wants to have a broad network of providers. Everyone wants to have an open formulary. Everyone wants to have the broadest benefits at the lowest cost without increasing their contribution every year.
Just by cutting a drug or a provider from your benefit may seem small, but the savings add up. (Like Big Bird or PBS.)
But, this is the problem we have in healthcare. How do we make enough small decisions to add up to real savings? How do we do this without upsetting everyone and impacting satisfaction (or is that simply life)?
October 5, 2012 0 Comments
The statistic that I like to point out is that more people have access to mobile devices than people who have access to toothbrushes. I know that sounds crazy to us Americans, but that’s apparently a global reality (in so much as statistics don’t lie). And, people seem lost without their smartphones so they have them within a few feet of them almost 24 hours a day.
Combine that with several trends, and you can begin to understand why Qualcomm Life predicts that by 2020 there will be 160 million Americans who will be monitored and treated for medical conditions remotely.
So, as I pointed out the other day about the value of the mobile data for a healthcare underwriter, that same data can be used to create a systemic intervention system for monitoring and intervening with consumers to drive behavior change. AND, since the data and delivery method is mobile, the interventions can be highly personalized based on when, how, what channel, etc. to improve engagement rates. I can even know who influences your behavior change and how to get them to encourage you to change behavior (peer pressure) or who you monitor and can influence you based on their recommendations.
I’m not sure I’m ready to go as far as Dr. Ron Loeppke from US Preventative Medicine who said
“These mobile apps that are emerging are going to be a predominant part of how health care is delivered going forward.” (Smartphones Take Wellness Engagement To New Levels by Elizabeth Galentine)
BUT, I do believe that over time that this will become the increasingly dominant channel for interventions and behavior change. Ultimately, your mobile phone number may be a more valued data point than your Social Security number.
October 5, 2012 0 Comments
There are so many attention grabbing ways of beginning this post…
Would you have guessed that all of these are talking about prescription drugs?
The Medicine Abuse Project (at www.drugfree.org) is trying to get this word out and find a way to change this. The basic points of their messaging:
October 5, 2012 0 Comments
I think we’ve all heard this at some point or another although I was surprised by the comparisons to the health values of sleep and working out. I wonder how hard I have to laugh to accomplish that.
Go Patch Adams!

October 3, 2012 0 Comments
Thus, the major factors that insurance companies traditionally use to charge higher premiums – such as health status, the use of health services, and gender – will no longer be allowed under the ACA. However, the ACA does permit employment-based health plans to charge employees up to 30 percent more on their premiums (and potentially up to 50 percent more) if they fail to participate in a wellness program or meet specified health goals. [From Kaiser document]
Traditionally, health plans and employers have rewarded consumers for taking some basic action (e.g., $100 for completing an HRA)…although some companies prefer penalties versus incentives.
At that same time, there is some evolution happening here with companies moving from simply paying for an action to requiring participation in a program (e.g., disease management). The next step that a few companies are engaging in is actually incenting or penalizing consumers based on health outcomes. This will certainly open some doors for legal challenges where people will argue that they are genetically pre-disposed to some factor that limits their ability to lose weight or lower their cholesterol or some other measure of health.
But, in one of the first legal challenges in FL, the court recently upheld the idea of rewarding (or penalizing) consumers based on taking a specific action (like completing a biometric screening). With that, I expect companies will be more empowered to take advantage of the fact that under health reform they can charge consumers up to 30% more for their healthcare for either not participating or not achieving a specific health outcome.
With an average monthly premium of $468 per month of single person coverage and consumers paying an average of 21% of their healthcare costs (or $97 per month), this means that a consumer could pay an additional $29 per month (or $349 per year). [If I interpret all of this correctly…if it’s 30% of the total health premium (not just the consumer’s share), then this jumps up dramatically.]
Not surprisingly, employees aren’t real excited about this. In a survey by the National Business Group on Health, 62% oppose charging employees more for health coverage if they do not participate in wellness programs. And, 68% oppose requiring employees to participate in a wellness program in order to qualify for health insurance.
And, according to the survey, the most effective cost control tactic was believed to be Consumer Driven Health Plans by 43% and wellness programs by 19% while 60% of employers plan to increase the premium paid by employees (i.e., cost shifting).
But, if companies throw out a life preserver (i.e., wellness program) to a drowing individual (i.e., unhealthy individual), why isn’t it a reasonable expectation that the individual has to grab it (i.e., participate in the program)?




