
I haven’t read the book yet, but this is a great video. I love the fast paced whiteboarding to match the speaking.
Archive | Research RSS feed for this section
DMAA Client Presentations
 July 28, 2010
July 28, 2010  0 Comments
0 Comments
We (Silverlink Communications) are very excited to see three of our clients get selected to present at DMAA this year. That is a tribute to all their hard work, creativity, inspiration, and willingness to leverage technology to improve outcomes.
Here are the presentation summaries from online:
Reducing Blood Pressure in Seniors with Hypertension Using Personalized Communications
CONTINUUM OF CARE SERIES
Wednesday, Oct. 13, 1-2 p.m.
- Examine how an integrated communications program that utilizes remote monitoring and interactive voice response components combine for an easily scalable, cost-effective solution to reduce hypertension.
- Review a program where 18 percent of participants transitioned their hypertension from out-of-control to well or adequate control.
- Identify best practices for how personalized, automated, interactive communications can be leveraged to control hypertension in a scalable manner.
- Evaluate how high blood pressure readings alerted patients with immediate feedback and education to help them better manage hypertension.
Improving Statin Adherence through Interactive Voice Technology and Barrier-Breaking Communications
Wednesday, Oct. 13, 2:15-3:15 p.m.
- Examine how interactive voice response (IVR) and barrier-breaking communications can measurably improve statin adherence.
- Review key barriers to statin adherence, including several barriers that are more significant than cost.
- Identify best practices for using IVR technology to improve statin adherence by addressing specific barriers.
- Evaluate how continuous quality improvement processes were used to drive higher response rates to IVR prescription refill reminder calls.
Addressing Colorectal Screening Disparities in Ethnic Populations
Thursday, Oct. 14, 12:30-1:30 p.m.
- Examine how interactive voice response (IVR) technology and personalized messaging improves the rate of colorectal cancer screening for different populations.
- Review the impact of ethnic-specific messaging on colorectal cancer screening rates and how this differs by ethnicity.
- Examine how engagement is influenced by the gender of the voice in communications outreach.
- Identify how to use predictive algorithms to project race and ethnicity to support tailored communications.
ADHD Drugs – Long Term Effect
July 24, 2010 0 Comments
Given the frequency of use of medications in our society today, I think there is much to learn once we see what happens when people are on medications for chronic conditions for their entire life.
Although this study only looks at 10 years and was funded by drug manufacturers, I think it’s a promising study that shows that kids that take stimulants for ADHD may have an initial slowing in weight and height, but that over 10 years there was no difference.
How Much Do You Really Notice?
July 24, 2010 0 Comments
The Dateline NBC show “Did You See That” shows us just how little we see or how easily our minds are distracted. This is a real issue when we think about communicating information to patients who have hundreds of other things going on in their life.
Would you notice if the man who stopped to ask you directions on the street all of a sudden became a woman?
Would you notice a man walking thru a group of basketball players when you were focused on counting passes?
Would you notice when the talk show host’s shirt turned from blue to green?
Would you notice that the person helping you at the store was blond one minute and a brunette the next minute?
People in the videos on the show didn’t. It was amazing…scary…surprising.
It makes you think. It made me want to experience the tests. Would I notice?
Watch this video – http://www.msnbc.msn.com/id/21134540/vp/38287250#38287250.
10 Numbers You Need To Know For Mobile Health
July 20, 2010 1 Comment
I found this great list of statistics yesterday from RxEOB. I won’t repost them all here so you click thru to the original content, but I thought it was very helpful.
23%. Percent of American households who use only a mobile telephone, no land line. Another 15% of homes with landlines report they receive all calls to their mobile device.
32%. Percent of Americans whom have accessed the internet from their mobile phone as of 2009. (19% reported they did it “yesterday”). In total 56% of Americans have accessed the internet via some form or wireless device (e.g., phones, MP3 players, laptop, game consoles).
81%. Percent of physicians will own a smart phone by 2012. Physicians are one of the highest using Smartphone demographics overall.
5,820. The number of health apps that were available for download from the major online Smartphone app stores (as of a report published Q2 2010).
66%. Percent of Americans who are interested in receiving health related emails from their health insurance company… 52% would be open to receiving emails that provide them feedback on their health process.
How Blunt Should You Be?
July 15, 2010 2 Comments

I’ve talked about this before from my personal perspective so I found this article about shocking men into going to the doctors right on point. But, I think this begs a great question…
“Should you communicate differently with men and women?”
My short answer is yes. In reality, it doesn’t always make a difference, but there are lots of times when it does. I’m not sure I’m ready to bet the farm on shocking messages to men all the time, but I would love to try that. Imagine an adherence message that told them they were improving their likelihood of death by 27% by not taking their medications. Or, a message about going to get a prostate exam which pointed out how many people die per year.
Most healthcare companies keep the gloves on when delivering messages. They are trying to motivate them, but they are hesitant to be too blunt (or direct). I’m sure that generally makes sense, but sometimes you just have to catch someone’s attention to get them to act.
Telling someone they are overweight and should start to workout and diet is very different than saying they are obese and are likely to die in their 50s if they don’t change their lifestyle immediately.
Related story – Top 5 Reasons That Men Don’t Go To The Doctor
Retail Rxs Filled By State (Sorted by Volume)
July 8, 2010 0 Comments
I found this 2009 data at the Kaiser Family Foundation site and downloaded it to sort it by state and show the percentage of scripts that are filled within the state (versus the total US script count). You should note that this is limited to retail claims (i.e., doesn’t include mail order Rxs).
| United States | 3,679,671,222 | |
| California | 312,440,433 | 8.5% |
| New York | 255,792,543 | 7.0% |
| Texas | 248,655,283 | 6.8% |
| Florida | 225,312,255 | 6.1% |
| Pennsylvania | 168,218,628 | 4.6% |
| Illinois | 156,310,649 | 4.2% |
| Ohio | 149,100,021 | 4.1% |
| North Carolina | 127,081,439 | 3.5% |
| Georgia | 119,238,095 | 3.2% |
| Michigan | 119,163,703 | 3.2% |
| Tennessee | 109,127,463 | 3.0% |
| New Jersey | 99,570,267 | 2.7% |
| Missouri | 92,754,941 | 2.5% |
| Massachusetts | 92,658,258 | 2.5% |
| Virginia | 90,704,636 | 2.5% |
| Indiana | 82,549,426 | 2.2% |
| Alabama | 80,669,107 | 2.2% |
| South Carolina | 75,527,841 | 2.1% |
| Kentucky | 73,756,811 | 2.0% |
| Washington | 66,329,432 | 1.8% |
| Wisconsin | 66,188,884 | 1.8% |
| Louisiana | 66,142,285 | 1.8% |
| Arizona | 61,297,786 | 1.7% |
| Maryland | 58,080,852 | 1.6% |
| Minnesota | 55,105,935 | 1.5% |
| Oklahoma | 48,972,975 | 1.3% |
| Arkansas | 48,242,080 | 1.3% |
| Mississippi | 47,735,160 | 1.3% |
| Iowa | 47,418,431 | 1.3% |
| Connecticut | 46,489,823 | 1.3% |
| Oregon | 40,342,008 | 1.1% |
| Colorado | 38,093,247 | 1.0% |
| Kansas | 36,214,744 | 1.0% |
| West Virginia | 34,432,644 | 0.9% |
| Nevada | 26,050,153 | 0.7% |
| Nebraska | 25,239,082 | 0.7% |
| Utah | 24,844,262 | 0.7% |
| Maine | 19,087,484 | 0.5% |
| New Hampshire | 18,033,822 | 0.5% |
| Idaho | 15,939,958 | 0.4% |
| New Mexico | 15,454,444 | 0.4% |
| Rhode Island | 14,723,946 | 0.4% |
| Hawaii | 14,249,708 | 0.4% |
| Delaware | 11,388,995 | 0.3% |
| Montana | 11,136,885 | 0.3% |
| South Dakota | 10,051,942 | 0.3% |
| Vermont | 9,682,741 | 0.3% |
| North Dakota | 8,404,232 | 0.2% |
| Wyoming | 5,991,536 | 0.2% |
| District of Columbia | 5,185,455 | 0.1% |
| Alaska | 4,488,495 | 0.1% |
Gender Bias – Postpartum Depression
July 8, 2010 0 Comments
We all know that females are different that males in terms of healthcare. And, regardless of the data, we all have biases in terms of what we believe. These biases can cause issues. (As I often say…”When you assume, you make an ass out of u and me.”)
That being said, I found the study a few months ago interesting where it said that 14% of American men develop depression either during their partner’s pregnancies or in the first year after delivery (peaking when babies are 3-6 months old).
This is important since depression is correlated with lots of health issues and has a family impact. The article mentions that children of depressed fathers have more emotional and behavioral problems than other kids at age 3 and more psychiatric disorders by age 7.
An interesting note was:
“Any healthy adult who goes without good sleep for a month is liable to become depressed.”
The big takeaway from the study is that physicians (and other healthcare entities) need to treat the family around birth. This is probably also a great opportunity for social media to support fathers as much of today’s infrastructure is set up to support the mother.
Wal-Mart Whitepaper on Restricted Pharmacy Networks
June 28, 2010 4 Comments
Of all the companies that might put out a restricted network whitepaper (PBMs, retail chains, consultants), I will admit that Wal-Mart is a surprise to me. It’s not that they haven’t been trying different strategies to increase market share – $4 generics, direct-to-employer contracting, but in general, I don’t see them doing a lot of marketing or selling in this space. They participate at one industry event, but their booth is very stark compared to other pharmacies.
But, that being said, the whitepaper makes the key points that anyone would make (i.e., I agree with the framing of the opportunity) with a slight twist of focusing on member savings versus payer savings.

Some of their key points from the whitepaper are:
- You should treat pharmacy negotiations like buying any widget. There is more supply than demand.
- Today’s model encourages all pharmacies to offer a rate that doesn’t get them kicked out of the network.
- Today’s model doesn’t encourage consumers to pick one pharmacy over another.
- There’s 5x more pharmacies than McDonald’s in the US…and no one would argue that it’s difficult to get a Big Mac.
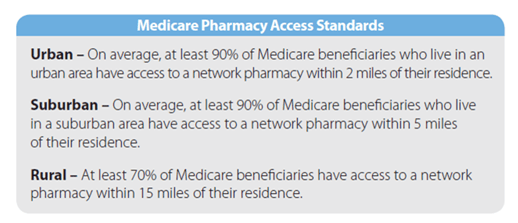
- They quote the Medicare pharmacy access standards to make the point about what access you can survive with. They reference an Express Scripts analysis that says the Medicare access standard can be achieved with a national network of less than 20,000 retail pharmacies (compared to the 60,000 in most networks).
While limited retail networks are not a new concept, they haven’t been widely adopted historically (<10% of clients). PBMs have always offered this type of plan design to payers – “If you remove a few chains from your network, you’ll get a lower rate from the other chains in return for increased marketshare.”
With the integration of CVS Caremark and their offer of Maintenance Choice, we’ve obviously seen the focus on this increase. And, the recent public negotiations with Walgreens highlighted that this is seen as a viable model for the future.
The question now is whether this will accelerate adoption of some type of limited network. If it goes forward, there are lots of questions to answer:
- How small will the network be – regionally, nationally?
- Who do you build the network around – CVS, Walgreens?
- What does this mean for mail order?
- What rates do the retailers have to match to participate?
- Does it include 90-day?
- Does the network start to look like a formulary where you have preferred pharmacies at one copay and non-preferred at another copay or is it either in-network or out-of-network?
- Does this increase or decrease power for the independents that have to be in certain places?
- Will anyone really test the national access standards and go to a 20,000 store network?
- What will consumers say and do?
- Does this accelerate adoption of cash cards and cash business for generics?
But, again, I struggle to see Wal-Mart as the chain that you build around unless the whitepaper is a thinly veiled attempt to push the direct-to-employer model (i.e., Caterpillar) which has saved the employer lots of money, but isn’t a simple to implement program (IMHO).
Here are some marketshare numbers for Walgreens, CVS, Rite-Aid, and Wal-Mart for the top 30 MSAs. Only 9 of those markets have Wal-Mart share above 10% and none are higher than 14%. For the other three, you have markets where they have a much higher concentration around which you can build.

Someone was asking me the other day if I saw the PBMs essentially partnering up. I’m not sure I do since there are markets where you would want to build a limited network with Walgreens and markets where you would want to build a limited network with CVS. At least for now, I don’t see Medco and Express Scripts just picking one dance partner although they might just based on who’s willing to play with them.
The other thing that becomes important here (tying this back to my Silverlink work) is communications. You have to identify who will be affected in moving to a limited network. You have to communicate with those people and help get them to the preferred pharmacy. You have to help them understand why you are doing this (savings) and WIIFM (what’s in it for me).
It creates some great dialog between the head of benefits and the CFO. We can save $X…BUT we will have to ask Y% of our employees and their families. Will they care? Do they know their pharmacist (unlikely)? Will it be an issue of convenience? Will they complain (of course…change is hard)? Will they ultimately care (unlikely as most disruption becomes accepted after 3-6 months)?
Does Age Matter in Adherence?
June 22, 2010 0 Comments
Certainly age could be a confounding factor for many reasons – health literacy, length with a condition, co-morbidities, number of medications, tolerance for side effects – but I like this chart that the people at Vitality (aka GlowCaps) (www.rxvitality.com or www.roseology.com) just put out.
Of course, like any survey, there is sample bias so I would hesitate to extrapolate this, but I would say something like…
“for people who have and use a refill reminder device in their homes for hypertension medications, older people are more likely to be adherent.”
Of course, I’d love to know their MPR (medication possession ratio) before using the device. Which had the higher lift?

Less Time in Hospital Correlated to More Readmissions
June 14, 2010 0 Comments
We all want to get out of the hospital as quickly as possible. A recent study from JAMA that appeared in the WSJ showed that while days in the hospital dropped from 8.6 days in ’93-’94 to 6.4 days in ’05-’06 the readmission rate (within 30 days) went up from 17.3% to 20.1%. I’d love to see the economics around this.
- Do the hospitals make more money in this case?
- Do the plans save more money?
- Are patients happier? [Remember that the majority of them got out sooner.]
“From a societal point of view, dollars spent on health care likely increased.” Harlan Krumholz, Yale University cardiologist and senior author of the study.

The study author echos a point that we [Silverlink] often make to our clients which is that hospitals (or payers) need to invest more effort and resources to make sure the transition to outpatient status in seamless. Do they understand what the doctor’s instructions were? Do they have someone caring for them? Did they pick up their medications?
Another key lesson learned here is that it’s important to measure what matters and that what’s measured gets improved.
2010 Medco Drug Trend Report
June 9, 2010 2 Comments
I can’t believe it’s taken me a few weeks to catch up on my notes from a conference call with David Snow and Dr. Rob Epstein from Medco Health Solutions about their 2010 Drug Trend Report. I captured some of Dr. Epstein’s comments in a quick blog post, but I have a lot of respect for David Snow and wanted to capture a few of his comments here and pull out some of the interesting data from the Drug Trend Report.
David Snow mentioned a few things:
- Reform has to address all three legs of the stool – Access, Quality, and Cost. Right now, it’s focused on access.
- Of the $2.4T we spend in the US on healthcare, $1T of it was unproductive.
- One of the big issues in the system is poorly designed systems for the people that deliver care.
- Pharmacy is ahead of the curve since it’s already wired and uses evidence-based care.
- We have to focus on the chronic conditions. 96% of the pharmacy spend and 75% of the medical spend is here.
- Prescriptions are used as first line solutions 90% of the time. (See my comments on why trend shouldn’t matter.)
- $350B of the waste is due to poor management of chronic solutions.
- We still have to address medical liability and defensive medicine.
He also answered questions. A few of my notes from the Q&A:
- Patent expiration doesn’t fully explain the increase in brand pharmaceutical costs. (Traditionally these drug costs go up once the patent expires.) You can correlate the tax on pharma (in reform) to the increase in prices. (Not dis-similar to the increases around Part D if memory serves me.)
- Adherence is a key issue. The Therapeutic Resource Centers (TRCs) are their answer to this. They drive adherence in the classes that matter and we report to clients on this. (While I think a lot of people viewed the TRCs as marketing strategies when they first came out, I believe they have demonstrated a clinical focus with some case studies and clinical leads over the past 18 months.)
- The pathway to biosimilars is very fair to the innovator.
- Class competition in specialty is increasing.
His most interesting comment which I’ll repeat from my earlier post was that if the FDA really understood true adherence they might make different decisions on approving drugs whose effect is tied to a person staying on a medication over time.
I won’t repeat some of the core data elements from my prior post, but here are some new ones from reading the document:
- Mail order penetration was 34.2% (which I believe is industry leading for the PBM sector with only Walgreens showing a 90-day utilization number that’s higher).
-
Interestingly, they show trend for clients with over 50% mail use (and clients with less than 50% mail use). [Most PBMs would love to have any clients with over 50% mail use.]
- 0.1% for those with over 50% versus 5.3% of those under 50%
Reported trends are based on 2 years’ data on pharmaceutical spending. Drug trend percent includes 201 clients representing approximately 65% of consolidated drug spending. The sample comprises clients who offer integrated (mail-order and retail) pharmacy benefit options for members. Clients with membership enrollment changes > 50% were excluded from the analysis. Plan spending is reported on a per-eligible per-month (PEPM) basis, unless otherwise specified. An “eligible” is a household, which may include multiple members who are covered under the same plan. Plan spending comprises the net cost to plan sponsors less discounts, rebates, subsidies, and member cost share. Generic dispensing rates and mail-order penetration rates represent the total consolidated Medco client base.

- Diabetes is obviously a critical category for everyone. I found it interesting that they saw fewer patients filing claims for diabetes but more drugs per patient in 2009.
- Respiratory therapies (driven by those <19 years old) jumped in contribution to trend from 8th to 2nd.
- In patients aged 35 to 49, antiviral drugs are the greatest contributors to cost – 8.3% of plan pharmacy costs. [Some of this driven by flu although this is not the at risk age group.]
Antiviral drugs (Formulary Guide Chapter 1.8) include oral treatments for HIV/AIDS, influenza, herpes, hepatitis C, hepatitis B, and injectable treatments for respiratory syncytial virus (RSV), and cytomegalovirus.
- Utilization growth for ADHD drugs for those age 20-34 grew 21.2%. [Is this for people not diagnosed as kids, people who have adult-onset ADD (if that exists), or just an over-diagnosis of the condition?]
- Specialty drugs…I’m always surprised that all the PBMs still have to caveat the fact that they only adjudicate some of the claims since some specialty drugs are filled and billed under the medical benefit. That seems like something that should / could be fixed, but I know it’s been tried and is hard since people are making money off them being billed elsewhere.


-
Cancer is already a huge driver of specialty costs AND:
- Much of the spending is still under medical;
- Most drugs approved in the past 4 years costs over $20,000 for a 12-week course; and
- There are over 800 drugs in the pipeline.

Spending growth has outpaced spending for nonspecialty, or traditional medications because:
- A high proportion of newly approved drugs are designated as specialty.
- Unique manufacturing processes make specialty drugs expensive to develop.
- Fewer drugs within a therapeutic category limit competition.
- There may be only one specialty treatment for an orphan condition.
- Few drugs are therapeutically equivalent to others in the category, reducing interchange and related cost savings opportunities.
- It is more difficult to transition existing patients from one specialty drug to another preferred specialty drug because often these drugs are large, unique proteins that are not considered interchangeable.
- Most small-molecule specialty drugs are relatively new with few generic alternatives.
- No defined approval pathway exists for follow-on biologics (also known as biosimilars).
- Drugs used to treat cancer represent a large portion of new drugs in both the pipeline and marketplace; most are specialty drugs and some can cost more than $20,000 for a 12-week therapy course.
- It was the first time I noticed anyone caveating the specialty trend. They proactively addressed different calculation methods to point out that their method yielded a 14.7% specialty trend, but if you did things differently (as I assume others must), then their trend would have been 12.1%.

- Trend in children exceeded trend in other age groups for the second year in a row. (I think this is an interesting perspective and a scary indicator for the future health of our country.)
-
They provided some examples of drugs that had new indications for younger patients approved:
- WelChol, Crestor—for low-density lipoprotein cholesterol (LDL-C) reduction in children aged 10 to 17 with heterozygous familial hypercholesterolemia.
- Atacand—for hypertension in children aged 1 to 17.
- Axert—for acute treatment of pediatric migraine.
- Protonix—for erosive esophagitis in patients aged 5+.
- Abilify—for irritability associated with autistic disorder in children aged 6 to 17.
- Seroquel—for schizophrenia in children aged 13 to 17, and for acute manic episodes in children aged 10 to 17 with bipolar I disorder.
- Zyprexa—for schizophrenia and for acute mania (bipolar I) in children aged 13 to 17.
- WelChol, Crestor—for low-density lipoprotein cholesterol (LDL-C) reduction in children aged 10 to 17 with heterozygous familial hypercholesterolemia.


- An interesting perspective that I’ve talked about many times (without the research capabilities to analyze) is the correlation between sleep and chronic disease. They looked at this across states based on drug utilization and found a correlation (not necessarily causation).

So what do they say to watch:
- Continued inflation in brand drug prices.
- Majority of trend will come from specialty – oncology, orphan conditions.
- Personalized medicine.
- Biosimilars.
- Generic pipeline.
- Obesity epidemic.

- They bring up an interesting issue relative to OTC (over-the-counter) product which is DUR (drug utilization review) which looks for drug-drug type interactions. They talk about the Medco Health Store integrating that data to monitor patients. [Do plans care? Do patients care? Should retail OTC purchases be integrated? How great are the interactions?]
-
They talk a little about obesity although I would love to understand more about how a plan sponsor should manage this.
- 68% of adults are overweight; 34% obese
- 32% of children are overweight; 17% obese
- Medical spending on obesity related conditions is $147B
- 19.5M adults (24-85) have diagnosed diabetes and other 4.25M are undiagnosed
- Diabetic medical claims are forecasted to grow from $113B to $336B over the next 25 years.
- I’m not going to spend a lot of time on personalized medicine here. (A recent post of mine on this topic.) They’ve been very active in this space for years talking about it. I think one of their interesting points in the Drug Trend Report is how Comparative Effectiveness will dovetail with Personalized Medicine.
- Almost 2/3rds of people at risk for CHD in the next 10 years and eligible for lipid lowering drugs (e.g., Lipitor) were still not using them. (A common gap-in-care program run by many companies is to target these people (e.g., diabetics).)
- Only 29% of patients treated for high cholesterol reach their cholesterol goal.
- They have a section on wiring healthcare which David Snow has talked about for a while. It’s a critical area to address and has lots of opportunity.
- They also talk about the concept of collaborative care (aka medical home…aka accountable care organizations).
- I’m a big believer that poly-pharmacy creates issues (as does poly-physician). I don’t hear much talk about it. I was glad to see them talk about a study they did which identified poly-pharmacy issues, talked to MDs, and ended up with 24% of cases where medications were changed.
A Medco survey reported that 81% of participants with a new diagnosis, who received services at a traditional retail pharmacy, either did not receive counseling or were dissatisfied with the prescription drug counseling they received. When given the opportunity to speak with a Medco Specialist Pharmacist, 75% of these patients accepted the offer of immediate telephone support.
- I thought it was really interesting to see a screen shot of their application used by the TRCs to create their Health Action Plans for consumers.

- I was also interested in their focus on women’s health and some data on caregivers and the gender differences in healthcare. One of their TRCs is dedicated to addressing these differences.

Do You Brush Your Teeth With Toilet Water?
June 4, 2010 0 Comments
While I hope not intentionally, this is a discusting reality for most of the world. Since most people flush with the lid up, the germs spread all over your bathroom. (One of the reason I hate those public toilets that auto-flush and cover you in germs all the time.) Here’s a good article on this along with a slightly humorous video below.
I was reviewing this list of worse places for your health that got me thinking about this. Here’s a few other highlights from the list:
* Don’t wear your shoes in the house and don’t store them in your closet.
* Don’t move hot food to the fridge to quickly or you’ll create a ripe environment for bacteria to grow.
* Don’t use the middle stall of a public bathroom.
* Don’t store your medicines in your bathroom.
* Don’t put your purse down on places you eat off. Nasty stuff on the bottom of those purses.
* Don’t use headphones in public areas with lots of background noise…you’ll turn the volume up so loud that you’ll damage your ears.
Should You Spank?
June 3, 2010 0 Comments
There was an article last month in Time (5/3/10) that caught my eye titled “The Long-Term Effects of Spanking“. I’ve never been a big fan of spanking, but I don’t have any issues with it either. I was spanked a few times as a kid, but it was the exception not the rule. I was surprised in another article to see that 22 states still allow spanking in schools. I would have an issue with that.
This article talks about a Tulane study published in Pediatrics magazine which says that children that are spanked may act out more in the long run. Those who were spanked at age 3 were much more likely to be aggressive at age 5. Apparently, this was the first study to control for issues such as depression, alcohol and drug abuse, spousal abuse, and whether the mother considered abortion. (All factors which apparently contribute to a child’s aggressive behavior.) Controlling for those, spanking still was a strong predictor.
“The odds of a child being more aggressive at age 5 increased by 50% if he had been spanked more than twice in the month before the study began.” Catherine Taylor, Tulane Professor
These children who had been spanked were more likely to be defiant, demand immediate satisfaction of their wants and needs, become frustrated easily, have temper tantrums and lash out physically against other people or animals.
The American Academy of Pediatrics (AAP) does not endorse spanking under any circumstances. They recommend time-outs which typically involve denying the child any interaction, positive or negative, for a specified period of time.
Any interesting discussion topic and one that for many us probably demonstrates the shifting winds of our culture. I don’t think I’ve ever discussed this with my pediatrician. I guess I know what her answer would be.
Some of my notes from RESULTS2010
May 28, 2010 0 Comments
This week was our [Silverlink Communication’s] annual client event – RESULTS2010 (click here to see the final agenda). I’ve talked about this before as one of the best events. It was great! Educational. Fun. Good networking.
Here’s a few of my notes along with a summary of the twitter feed (using hashtag #results2010). Unfortunately, the two of us twittering were also fairly involved so there are some gaps in coverage. And, my notes are sporadic due to the same issue.
Overall themes:
- Communications are critical to driving behavior change.
- We have to address cost and quality.
- Reform creates opportunity.
- Systemic problems require systemic solutions.
- Measure, measure, measure.
- Automated calls – while not the whole solution – work in study after study.
- People are different.
- There is a gap in physician – patient interactions.
Notes:
- Reform basics – guarantee issue, requirements for coverage, income related subsidy.
- Independent payment advisory board has an aggressive goal – get Medicare spending to equal GDP growth + 1% each year.
- ½ of the $1 trillion needed to pay for health reform comes from Medicare savings / reform…the rest from taxes.
- Everyone’s fear is that MCOs become “regulated utilities” that just process claims…unlikely.
- Need to address underuse, misuse, overuse, and limited coverage.
- Need to measure quality and cost at the person level.
- CMS pilots around shared savings are working – outcomes improved.
- Medicare Part D only got one complaint per thousand for therapeutic interchange programs / drug switching.
- The decision around defining MLR (medical loss ratio) and what fits in there is critical.
- Healthcare is like anything else…it’s not great and needs to change, but don’t touch mine cause it works ok. [frog in the pot]
- How do we make each healthcare decision an informed decision.
- Decision aids.
- Pull, push, or pay – 3 ways to drive awareness.
- Moving from information about your care to information being care.
- The incentive rebound effect…what happens when you take away an incentive.
- Social interaction affects our behavior.
- Solving for how to change consumer behavior cost effectively and in a sustainable manner is a good challenge to work on.
- How do we move people from desires to action? From “I’d like to exercise” to actually doing it.
- The fact that some European programs take 3-5 years to see an impact makes me wonder what that means for our US investment strategy given the member churn across plans.
- Great examples of ethnographic interviews
- Good McKinsey data on people’s perceptions – Annual Retail Healthcare Consumer Survey.
- Inform / Enable / Influence / Incentivize / Enforce
- One way of categorizing – willingness to change versus barriers to change (rational, emotional, psychological).
- Attitudinal segmentation – cool…but how to scale?
- Provider staffs attitudes are important.
- Design – delivery – measurement
- Readiness to coach
- A culture of health
- Have to mix up your tools (incentives, channels)
- “Communication Cures”
- The chief experience officer is a new role in plans and PBMs.
- The only experience you have with health insurance is via communications. Make it count.
- Loyalty is a result of cumulative experiences.
- People have to trust you so they listen to your message
- Communication maturity model
- Price is what you pay; value is what you get. (Warren Buffett quote…he wasn’t there)
-
Shifting paradigms:
- Consumption to sustainability
- Possessions to purpose
- Retirement to employment
- Trading up to trading off
- Perceived value to real value
-
Simple…less is more
- 1/3 of people feel their lives are out of control.
- Inflamation causes 80% of diseases (really)?
- If only 10% of outcomes are driven by costs, why do we spend 100% of our time trying to fix that problem. [tail wagging the dog] [It’s the same point on adherence.]
- There are 45M sick days per year from 5 conditions – hypertension, heart disease, diabetes, depression, and asthma.
- Have to look at clinical efficacy and elasticity of demand.
- Commitment, concern, and cost.
- Five components – plan design, program, community, communication, and provider engagement.
- Need a multi-faceted approach to create a culture of health.
- MDs much more likely to talk about pros than cons.
- There would be 25% less invasive procedures if patients fully understood the risks.
- Foundation of Informed Decision Making
- Huge gaps in patient view versus physician views around breast cancer.
- Preference-sensitive care
- Dartmouth Atlas
- Genomics tells you the probability of being on a disease curve, but not where you are in the potential severity.
- Only 60-70% of women get at least one mammogram their entire life.
-
Statin study – barriers to adherence:
- 37% didn’t know to stay on the Rx
- 27% side effects
- 15% convenience
- 15% MD instructions
- 11% cost
- In healthcare, we’re all taught to speak a language that no one else understands.
- It takes a village.
- Challenge – Use communications to cure cancer.
- Collaboration. Innovation. Evaluation.
- Adherence is a great example of where everyone’s interests are aligned.
- There is no magic bullet for adherence.
- You need a multi-factorial approach to address adherence…Physicians are rather ineffective at addressing adherence.
- Evidence-based plan design works to impact adherence (although I think another speaker said no).
-
You have to think about operant conditioning. (Look at dog training manuals and kid training manuals – very similar)
- My example here is using clicker training for humans.
- Think about all the failure points in the process.
- What is the relative value to the patient.
- Reward system has to reward at the failure points not just at the end of the process.
- Using a point system successfully increased the use of a select (on-site) pharmacy by 57% at one employer.
- 75% of PBM profits are from dispensing generics…that’s why Wal-Mart was able to be a threat to the industry.
- Drugs only work in 20-80% of people.
- There are people with a gene that doesn’t break down caffeine.
- 3% of people are ultrafast metabolizers of codeine (which turns to morpheine in the body)…that can be a problem.
- Epigenetics – turning DNA switches on and off.
“Tweets”
Rebecca from ProjectHEALTH closes #results2010 with a remarkable talk on this crucial program; they work with 5,000 families/year.
Reid Kielo, UnitedHealth: 93% of members validated ethnicity data for HEDIS-related program using automated telephony #results2010
25% of Medco pt take a drug with pharmacogenetic considerations. Robert Epstein, CMO Medco #results2010
Bruce Fried: the “California model” of physician groups facilitate efficiencies that improve delivery; an oppty for M’care #results2010
Bruce Fried on Medicare: 5 star ratings have strategic econ. importance, med. mgt. and cust serv. key #results2010
Fred Karutz: members who leave health plans have MLRs 2 standard deviations below the population. #results2010
Fred Karutz: Market reform survival – retain the young and healthy #results2010
Poly-pharmacy has negative impact on adherence. #cvscaremark
#results20101 in 3 boys and 2 in 5 girls born today will develop diabetes in their life. SCARY! #results2010
20% of all HC costs associated with diabetes. #results2010. What are you doing to manage that?
Messages to prevent discontinuation of medication therapy far more effective than messages after discontinuation. CVS #results2010
25-30% of people who start on a statin don’t ever refill. #CVSCaremark
#results2010Maintenace of optimal conditions for respiratory patients increased 23.4% with evidence-based plan design. Julie Slezak, CVS. #results2010
Value-based benefits help control for cost sensitivity for medications; every 10% increase in cost = 2% – 6% reduction on use. #results2010
Pharmacists who inform patients at the point of dispensing are highly influental in improving adherence. William Shrank #results2010
The game of telephone tag in HC is broken. Pt – MD communications. #results2010
37% of Pts were nonadherent because they didn’t know they were supposed to keep filling Rx. #results2010
Last mile: 12% of Americans are truly health-literate; they can sufficiently understand health information and take action. #results2010
Only 12% of people can take and use info shared with them. #healthliteracy
#results2010
#DrJanBerger.We need to improve the last mile in healthcare… clear, effective conmunication. Jan Berger #results2010
#McClellan used paying drug or device manu based on outcomes as example of “accountable care”. #results2010
72% of those with BMI>30 believe their health is good to excellent; as do 67% of those w/ chronic condition. #McKinsey
#results2010Are incentive systems more likely to reward those that would have taken health actions anyways (i.e., waste)? #McKinsey
#results2010
Only 36% of boomers rate their health as good to excellent. #results2010
27% of people believe foods / beverages can be used in place of prescriptions. #NaturalMarketingInstitute
#results2010Why do we spend so much time on impacting health outcomes thru the system when that only explains 10%. #Dr.JackMahoney #results2010
Using auto calls vs letters led to 12% less surgeries & 16% lower PMPM costs in study for back pain. #Wennberg
#HealthDialog
#results2010MDs are much more likely to discuss pros with patients than cons. #Wennberg
#HealthDialog
#results2010Should physicians be rewarded as much for not doing surgery? How do economics influence care decisions? #results2010
Physicians were 3x as concerned with aesthetics than breast cancer patients in DECISIONS study. #results2010
Fully-informed patients are more risk-averse; 25% fewer of informed pts in Ontario choose angioplasty. #results2010
Patients trust physicians over any other source (media, social connections) but only receive 50% of key knowledge. #results2010
Informing Patients, Improving Care. 90% of adults 45 or older initiate discussions about medication for high BP or cholesterol. #results2010
What is #results2010? #Silverlink client event.
#results2010 – #Aetna Medicare hypertension program leads to 18% moved from out of control to in control using auto calls (#Silverlink) …
About 2 of 3 medicare pts have hypertension. #results2010
John Mahoney describes how he connects payors, providers, and care via research. #results2010
As information becomes commoditized in healthcare, sustainability enters the vernacular. #results2010
Segmentation innovations of today will be tomorrow’s commodities. Measurement and learning must be “last mile” IDC insights #results2010
Plans are strategically investing in bus. intel to reach wide population for wellness, not just the low-hanging fruit. #results2010
The single most significant future market success factor is measurable results. Janice Young, IDC Insights. #results2010
Knowing our attendees’ preferences could have fueled segmented, precise invitations to #results2010. Dennis Callahan from Nielsen Media.
Drivers of those sereking alternative therapies: stress, lack of sleep and energy, anxiety, inflammation. #results2010
Only 2% of people don’t believe it’s important to lead a healthy lifestyle. Their behavior could’ve fooled me. #results2010
Are purity and simplicity the new consumption? Steve French of Natural Marketing Institute explores. #results2010
Gen Y is the most stressed out generation. #results2010
Less is more. 54% say having fewer material possessions is more satisfying. Natural Mktg Institute #results2010
Loyalty is a result of a cumulative set of experiences. Individual intervention ROI is sometimes difficult. #results2010
Sundiatu Dixon-Fyle of McKinsey; understand how beliefs shape an individual’s ability to change behavior. #results2010
Don Kemper: each of 300M HC decisions made each year need to be informed. #silverlink
#results2010Medicare Part D: 40% lower cost than projected, seniors covered through tiered coverage powered by communication. #silverlink
#results2010Mark McClellan: Brookings is engaging private insurers to pool data to understand quality of care. #silverlink
#results2010Mark McClellan at RESULTS2010; bend the curves, provide quality care efficiently. HC reform >> insurance reform. #silverlink
#results2010





Medco 2010 Drug Trend Report
May 19, 2010 1 Comment
Today, Medco Health Solutions released their 2010 Drug Trend Report (which looks at 2009 data). I haven’t had time to read the entire report, but here are a few highlights and comments from a conference call:
-
Overall drug trend was 3.7%. [They use their top 200 clients for analysis.]
- Trend was 0.1% for clients with greater than 50% spend at mail.
- Trend was 1.7% for Medicare.
- [I still point out here that the question is whether trend is good or bad.] Dr. Epstein and David Snow pointed out that they work with clients on this to track metrics on adherence at the TRCs (Therapeutic Resource Centers) and report on this. The key here is knowing what classes show measurable impact to overall costs and outcomes by improving adherence and increasing costs.
- Another point I thought was interesting was a comment that if the FDA saw the actual adherence on some drugs that require sustained utilization to achieve an outcome that they might make different decisions about drug approvals.
-
Inflation for branded drugs was 9.2% which was the highest in a decade. Generic inflation was 0.3%.
- On a conference call, David Snow validated that this was associated with the tax on brand pharma so yes the high inflation on brand drugs was tied to reform. Someone asked a question about patent expiration (which historically drives prices up), but that doesn’t explain all the inflation here.
- They saw a 3.4% increase in generic utilization.
-
Prescription utilization was up a minor 1.3%.
- 5% for children 0-19.
- 0.2% for seniors.
- Specialty drug spending continued its rapid growth with a 14.7% increase including a 2.6% utilization increase.
- Diabetes continues to be the largest driver of drug trend representing 16.7% of all drug spending and grew by 11.1%. [We can expect to see this continue to grow as more pre-diabetics are diagnosed.]
- H1N1 drove up antiviral spending by 15.7%.
- Pediatric use of medications grew faster than other groups.
- 1 in 4 insured kids now take a medication for a chronic condition.
-
Increased utilization in kids occurred in diabetes, asthma, antivirals, ADHD, cancer, and rheumatology drugs.
- There was a huge increase in diabetes over the decade (5x the adult population) and this was especially true with adolescent girls.
- It’s amazing to me that you now have kids on lipids (high cholesterol), but it’s clearly an indication of the obesity issue. [We’re just at the tip of iceberg.]

-
ADHD surged for those under 35 – 9.1% increase in use leading to a 23.8% increase in spending.
- The CDC says that 5M kids age 3-17 have and ADHD diagnosis.
- [The other issue here is abuse of ADHD drugs.]
- They also mention Nuvigil as a drug that could gain popularity for treating jet lag.
- They forecast the drug trend will rise 18% thru 2012 driven largely by diabetes, oncology, and rheumatology.
- About $46B in brand drug sales are scheduled to go generic by 2012.
- They don’t expect biosimilars to impact the market until after 2012.
- Not surprisingly, they showed a high correlation between states with frequent sleep deprivation and high drug utilization. As I’ve talked about many times, lack of sleep drives obesity which is highly correlated with many conditions. They also found a notable overlap of the use of Provigil (as stimulant used to treat daytime sleepiness associated with sleep apnea). [Seems like a drug that could get abused by college students like ADHD.]
“While H1N1 caused a spike in antiviral use among children last year, the far more alarming trend since the beginning of the decade is the increasing use of medications taken by children on a regular basis and in some cases, for conditions that we don’t often associate with youth, such as type 2 diabetes,” said Dr. Robert S. Epstein, Medco’s chief medical officer and president of the Medco Research Institute. “The fact that one-in-three adolescents are being treated for a chronic condition points to the need for additional health education and lifestyle changes that can address the obesity issue that is likely a driving force behind such conditions as type 2 diabetes and even asthma.”
If you’d like to get updates whenever I post on the blog, you can sign-up for e-mail updates here.
Automated Call Nudge – WSJ
May 19, 2010 0 Comments
Yesterday’s WSJ had an article about some research done at Stanford about comparing automated calls and human interventions. The goal was to see what motivated people to exercise more. As you can see in the chart below, at 6-months automated calls produced better results while at 12-months they were below the human interventions. But, an automated solution is obviously much more cost efficient and scalable. The one big question I have is how to make the automated calls even more interactive. There are lots of things we do at Silverlink to use automation to drive behavior.
While many are skeptical, the reality is that automated calls are the best channel in healthcare based on the cost per success ratio. [Do you know any other channel that can get you a 70% “open” rate?] You can deliver PHI. You can track interventions for audit purposes. You can have real-time access to data. You can create rules based solutions that dynamically change based on interactions.
And, this is not the first study Stanford has done on this. Here’s links to two older studies they did:

Who’s Your Date To The Genetic Testing Prom?
May 18, 2010 1 Comment
Genetic testing (aka pharmacogenomics, personalized medicine) is certainly a hot topic these days. There is lots of research around how to use the testing to manage drug spend by appropriately matching drugs with genetics at the individual member level.

I find it interesting to see who’s going to the “prom” with whom here. Another interesting perspective is how physicians feel about these (see survey).
- Medco acquired DNA Direct.
- CVS Caremark hired Per Lofberg from Generation Health and invested in the company.
- P&G invested in Navigenics.
- Walgreens was going down the path with Pathway Genomics before the FDA intervened.
So…what is Express Scripts doing? I’ve heard some talk at a conference about their strategy which involves a broader focus on integrating data from multiple sources including genetic testing to help drive clinical decisions. It seems like they’re either late to the party or smart in staying away. The question is whether this is a nice to have, a differentiator, or something that consultants will start requiring the PBM to provide. From their 2009 Outcomes conference:
[Genomics and personalized medicine] The potential for improved outcomes and cost savings are attractive but still unproven.
Don’t Believe The Hype – Copay Waivers
May 11, 2010 0 Comments
 Don’t believe the hype – its a sequel
Don’t believe the hype – its a sequel
As an equal, can I get this through to you
I talk about it all the time as most people do…non-adherence to prescription drugs is a real issue. People don’t fill their initial script. People who do fill their first script drop off after the first several fills. By 12-18 months after a patient starts therapy, less than 50% of them are still taking their medications. Here’s a few key articles on this:
Common barriers to adherence are under the patient’s control, so that attention to them is a necessary and important step in improving adherence. In responses to a questionnaire, typical reasons cited by patients for not taking their medications included forgetfulness (30 percent), other priorities (16 percent), decision to omit doses (11 percent), lack of information (9 percent), and emotional factors (7 percent); 27 percent of the respondents did not provide a reason for poor adherence to a regimen. Physicians contribute to patients’ poor adherence by prescribing complex regimens, failing to explain the benefits and side effects of a medication adequately, not giving consideration to the patient’s lifestyle or the cost of the medications, and having poor therapeutic relationships with their patients. (NEJM article)
Depending on what study you look at cost is certainly an issue, but it typically isn’t the primary issue. I typically see cost as being a factor in 5-15% of the cases. I think if you look at how Merck weighs cost in their Adherence Estimator that it is only a small factor. A lot of this plays out in VBID (Value Based Insurance Design) which while not purely about copay waivers that certainly is an element of most solutions.
A few friends of mine formed their own company (CareScientific) and had a paper published in AMCP recently. From that article:
VBID is receiving attention as a tool to increase medication adherence and lower medical costs. However, applying a “plausibility calculation” method to data generated from a recent VBID study involving reduction of drug copayments, this evaluation found that health plan sponsors are highly unlikely to experience net savings by implementing VBID programs, even under generous assumptions, for 2 reasons. First, the price elasticities of medications are too low to generate meaningful increases in medication adherence when copayments are lowered. Second, the potential reductions in the avoidable hospitalization and ER utilization rates across a commercially insured population with varying risk levels are generally not large enough to offset the additional plan costs of lowering copayments to increase medication adherence.
I would also suggest looking at some of their tools that they’ve developed.
So, getting back to how I’m tying in my reference to Public Enemy (rap musicians)…
When I look at the upside for pharmaceutical manufacturers to grow the pie (get more Rxs through adherence), I often wonder why one of the default solutions is to fund copay waivers. That happens by employers, health plans, and even the manufacturers. There are many less expensive ways to get that lift by addressing things like reminders and tailoring information to individuals based on their personalized barriers.
There are lots of high cost solutions that will make an impact. The question is how to triage those resources to focus them on the right people. It’s important to identify adherence risks (pro-active intervention) and adherence gaps (retrospective) and intervene with the patient.
Here are a few of my other posts on this:
- How Does Adherence Fall Off?
- Adherence Estimator by Merck
- Adherence Graphic
- More Adherent if You Use Mail
- Should Drugs Be Free?
- Sick Patients = More Rxs = Lower Adherence
- Adherence Examples of Communications
- Managed Healthcare Executive
- Single Answer or Multiple Answers
- Concise Summary of Compliance Reality
The Facebook and iPod Generation
May 5, 2010 1 Comment
When I think of the current generation that is coming into the workforce, I think of people who:
- Grew up with social media all around and are less concerned about privacy
- Grew up with the ubiquity of technology having an iPod always on and being in constant communication with their mobile phone
- Grew up with the US in a constant state of war – 9/11, Iraq, Afghanistan
- Grew up with the idea of constant stimulus – portable video games, TVs in the car
- Grew up with periods of market instability – technology bubble, 9/11, housing bubble
- Grew up with a likelihood of living at home after college [and think that’s ok]
- Grew up with more global awareness via CNN and the Internet
- Grew up with allergies and general paranoia – no more leaving home as a kid and coming back when the sun set or eating peanut butter at school

I think the more typical perception of many of them is an overly privileged generation who can’t focus on one thing, expect everything (money, position, title, responsibility) regardless of whether they deserve it, don’t follow basic protocols (like a thank you after an interview), have been coddled their whole life, and have no respect for what others have done. But I think every generation thinks that of the next generation.
I guess the official definitions are: (see good presentation)
- Traditionalists – born before 1946
- Baby Boomers – born btwn 1946 and 1964
- Generation X – born between 1965 and 1981
- Millennials – born 1982 to 2000
The Millennials are also called Generation Y, GenNext, the Google Generation, the Echo Boom, or the Tech Generation and are 76M strong. With immigration they are likely to surpass the Baby Boom generation in the 2010 census. [Note – Comments derived from reading an exerpt of The M Factor by Lynne Lancaster and David Stillman in the May 2010 Delta Sky Magazine.]

Their book – The M Factor – is focused on this generation. They talk about the fact that this generation is talking about and searching for “meaning” in their work. They’ve been raised by working parents that struggled with life balance and want more out of work for their kids. They see how work has become so engrained in our lives with Blackberries and other tools.
More than 90% of US Millenials said having opportunities to give back thru their company was somewhat to very important when considering joining an organization.
51% of young workers surveyed as part of the Kelly Global Workforce Index were prepared to accept a lower wage or lesser role if their work contributes to something “more important or meaningful”.
The question that a lot of this drives at is how do you leverage the passion and tech savvy Millenials as part of your workforce. They are going to drive changes. They are going to be innovators. And, they’re not going anywhere. Here’s a good blog on Generation Y.
It reminds me of some mock interviews I did a few years ago at my business school. I was stunned by some of the accomplishments of these people. They had founded companies and businesses. They had volunteered in the community. They were well read and had passion for things that I didn’t care about at their age. I was glad to have made it thru school with my peers. But, on the flipside, I talked with my friends who are the Dean of the School and run the Career Center to point out that not one of those people wrote me a thank you or sent me an e-mail. None of them ever asked me to help them find a job leveraging my network.
The article talks about this Millenial generation growing up at a time when the divorce rate had dropped and parents spent more time with their kids and transformed from authority figures to mentors and friends of their kids. This whole concept of “helicopter parents” has been explored in other areas and still amazes me. [Are you a helicopter parent test.] For example, 11% of US Millenials said they would feel comfortable involving their parents in salary negotiations. [If I had the option legally and a parent showed up with their kid for a salary negotiation, I would rescind the offer. If they can’t do that by themselves, how can I trust them to drive my business in pressure situations?]
In healthcare, the best example I always use for a company focusing on this generation or the “Young Invincibles” is Tonik Health which is a Wellpoint brand. I’m always surprised how few people know them. Take a look at their website (below) – the colors, the words, and the positioning is all so different than how most of us think about our health insurer. Here’s a good blog entry on the “millennial patient“.

Why is this relevant to my healthcare communications blog – because segmentation is so key to effective messaging. You have to understand this generation and how to engage them and drive them to take care of their health. Traditional language, modes, techniques, and messages may not work. The article (from the book) talks about their focus on feedback and scoring. They are used to constant [positive] stroking and having a score to evaluate success. They grew up being rewarded for everything. How does that manifest itself in a wellness system that tracks their good deeds (exercise, diet, preventative actions), provides them with rewards, frames their effort as contributing to the greater good, and integrates technology (e.g., connect devices)?
Only 3% of the people they surveyed said that Millenials handled negative feedback well. They haven’t been allowed to fail. This makes me think about one of my favorite quotes from IDEO – Fail Often To Succeed Sooner. You have to understand how to try, fail, learn, and try again to make improvements.
Here’s some recent research we’d done at Silverlink on the “young invincibles” and “Why I Have Health Insurance”:

Implications of Frugality as the New Black
May 5, 2010 0 Comments
I have heard some dialogue about consumers freeing up their spending even without their salaries going up or their house value going up (although their portfolio may have recovered by now). But, the question is how the frugality that was learned in the past year will impact consumers long-term. Will it change the way they buy? Will that be true across generations or will this just have a major impact on certain generations that are just coming of age?
An article released by Booz & Company a few weeks ago has some interesting data in it. For example, in the chart below, it shows 22% of people spending less on healthcare (drugs, supplies). What does that imply – pill splitting, more generics, more mail order, lower adherence, less preventative care? So are they more receptive to cost messages from healthcare entities?

Most of the consumers surveyed said they continue to consider saving more important than spending (65 percent). They sacrifice convenience for price (65 percent), frequently use coupons (65 percent), and, to a lesser extent, prefer the best price to the best brand (55 percent).
Maybe it’s time for the PBMs to emphasize convenience more – simplify your life, use mail order…one less errand to run. I’m still skeptical that this would beat a traditional cost savings message. BUT, perhaps it’ time to reconsider coupons / incentives. They’ve been tried with limited upside over the years in pharmacy. They do drive up results, but they don’t always pay for themselves. Maybe a lower value incentive would have the same yield thereby increasing ROI. ???
They identify six segments of the population with this frugality filter:

Thoughts On Express Scripts 2010 Drug Trend Report
May 1, 2010 0 Comments
As one of my favorite annual projects during my time at Express Scripts, I love the drug trend report. It has been a historical benchmarking tool for the industry and become a normal deliverable for many of the PBMs. Here are my initial thoughts after reading this year’s document which looks at 2009 data.
Individuals often are not rational.
- As driven by their Consumerology initiative over the past few years, Express Scripts has shifted the dialogue around the B2C components of the PBM industry to one of behavior change versus simply plan design. This report continues to reinforce that messaging.
- Waste has been an ongoing drum beat since my days there. This continues to be the message with a shift to include non-adherence to channel mix and drug mix.

- They talk about the Healthy People 2010 initiative and that key to closing “the last mile” in achieving our objectives is the ability to influence behavior.
- One of my favorite charts is below showing the waste by class. Not surprising, plan sponsors should focus on heart disease, depression, high cholesterol, and ulcer disease. [Diabetes is not in the top four but is one of the typical areas of focus.]

-
Key Performance Indicators (KPIs):
- Overall drug trend – 6.4%
- Specialty drug trend – 19.5%
- Traditional (non-specialty) drug trend – 4.8%
- $800.23 PMPY average drug spend
- The top five classes are:

- Specialty drug spend is up to $111.10 (processed under the prescription benefit) with a belief that this is only 50% of the total spend which includes specialty drugs processed under the medical benefit.
- The top specialty classes include inflammatory conditions, MS, and cancer which represent 67% of total specialty spend.
- I was surprised to see the member contribution to the drug costs had gone down while the actual dollars had stayed flat.

- I was also surprised that they found adherence (as measured using Medication Possession Ratio) stayed flat from 2008-2009. I think most of the information available had implied thru survey data that it was going down with the recession.

- I’m having some difficulty reconciling the MPR analysis below with the waste argument. If 80% MPR is ideal and most classes are above 80% MPR, I’m not sure I see the crisis in the data.

- One of the key charts that I always copied and hung on my wall is the one below. It shows the classes by rank, the utilization, the average cost, and now the estimated behavioral waste (generics and mail).

- You should certainly go into the document and look at the class level detail. They’ve included a utilization chart by gender by age which I really like. The sections also give some insight into future pipeline. I think I’ll pull diabetes out into a separate post.
-
It’s interesting that they identify only three segments for non-adherent patients with specialty medications versus more on the traditional side:
- Active Decliner
- Refill Procrastinator
- Sporadic Forgetter
- They project that utilization will continue to go up at about 3% per year and that trend will be mitigated with new generics coming to market.

- Another interesting analysis is where the waste is by state:

- They have some information on their Consumerology approach, but I’ve talked about that before.
- I liked their simple plan design primer:

-
Towards the end, they talk about some of the changes they’ve made over the past few years to their programs to reflect their consumerism approach:
- Step Therapy Choice
- Formulary Rapid Response
- Call4Generics
- Select Home Delivery (which is gem of their new programs in my assessment)
- First Generic Fill Free
- Select Curascript
- A simple graphic that points to the importance of understanding the consumer and developing programs to effectively drive behavior is below. [This is very similar to all the work we do at Silverlink with clients to help them drive health outcomes and behavior.]












I like it. Very humanized versus purely statistical document. Good job Emily, Steve, Yakov, Andy, Bob, Brian, and Chris. (That’s the core group that I know well.)
How Does Adherence Fall Off?
April 29, 2010 0 Comments
This is a nice simple graphic from a new Medco document that’s out – Case For Smarter Medicine. We all know adherence is an issue especially in the first 3 months (for those that ever fill even their drugs one time), but this gives us a good picture of how it drops off over the first 12 months.

The Best Healthcare Conference
April 28, 2010 1 Comment
In today’s budget conscious economy, people are constantly evaluating where to spend their time and money from a conference perspective. Some conferences are good networking events. Some of requirements to work in an industry. Some are educational. Some give you new ideas on how to run your business. Some are in great fun locations with fun events. Very few fit all of those.
I think our Silverlink Communications client event called RESULTS2010 does all of those. [Hint – the conference is called RESULTS since that’s what we focus on with our customers.] It takes on all the key issues we see in the market. It brings in industry experts and clients to talk about what they are doing to address these issues. Those problems are framed out by our industry experts that have line experience with these roles. [Our leadership team comes from places such as Express Scripts, CVS Caremark, Gorman, and HCSC and our team includes people from McKesson, Humana, United Healthcare, IMS, DigitasHealth, Medco, and WebMD. I challenge anyone to find a more knowledgeable vendor team.] It gives people a chance to network and talk to their peers. And, there’s some fun mixed in there.
This year’s event is focused on THE HEALTH CONSUMER. I’m pretty sure it’s the only conference focused on communicating with consumers in healthcare. The objective is to provide clients with ideas about how to educate, support, and motivate consumers to take actions which support health outcomes.
Honestly, it was the original event that convinced me to come to Silverlink. I was a consultant at my first event working with the company. I met 75 users who were passionate about the company and had great first hand experience using the technology to make a difference in their companies. I was able to ask them about the competition and understand why they choose Silverlink for their member communication partner.
So, what does this year’s event have in store:
- An amazing list of external speakers including Mark McClellan, David Wennberg, Don Kemper, Jack Mahoney, and Janice Young.
- A long list of client case studies – 14 so far.
- Specific tracks to cover our different client groups and allow for smaller discussion versus formal presentations – Pharmacy, Population Health, Medicare, and Managed Care.
- Industy experts on key topics such as consumer engagement, use of data in healthcare, consumer data, behavior change models and incentives, pharmacy economics, pharmacogenomics, medicare market dynamics, and the evolving retail healthcare model.
- Adherence experts such as Dr. Will Shrank from Harvard and Valerie Fleishman who led the NEHI adherence study that is widely quoted.
- Several fun events including golf, morning runs, and a few special sports related surprises.
There are several more speakers who you would know and I’m very excited to have come and speak…BUT, I want to leave something inside the package for you to want to rip it open and learn more.
How much does it cost? Nothing (as long as you’re a Silverlink client).
Where is it? Boston (a great city).
How do I learn more? Well…if you work for a large managed care company, a population health company, or a pharmacy / PBM, you may already be a client. We have over 80 clients today. So, if you’re not on our invite list, think you might be a client, and want to learn more, let me know. I’m at gvanantwerp at silverlink dot com. [spelling it out avoids spam]
This year’s event is in late May so I hope to see many of you there!
Would You Like Some Food With Your Salt?
April 28, 2010 0 Comments
This is a good example of too much of a “good thing”. The recommended daily salt maximum is 2,300 milligrams. But, men consume 4,300 mg per day and women consume 3,003 per day (National Health and Nutrition Examination Survey).
What’s the problem? Excessive sodium can lead to high blood pressure which is associated with strokes, kidney damage, and congestive heart failure. The Institute of Medicine estimated that reducing sodium intake could prevent 100,000 deaths a year and save $18B in medical costs.
And, salt also contributes to the obesity crisis by creating a brain response that craves more and causes people to drink more soft drinks and alcoholic beverages. Some big claims.
Prescription Growth Trends March 2010
April 26, 2010 0 Comments
These charts from IMS and Barclays Capital show 0.9% script growth for 2010 YTD. Retail continues to grow while mail continues to decrease volume.


So, I guess the question is what to make of this. Is it right?
- IMS doesn’t get all the data (e.g., Wal-Mart and I think some mail order data).
- The independent pharmacies all complain about the PBM’s taking business away. This would say that’s not true.
Let’s just take Express Scripts as an example. In 2004, Express Scripts filled 39.1M mail Rxs out of 437.8M total claims. In 2009 (after the Curascript, Priority, and MSC acquisitions), Express Scripts filled 41.8M mail and specialty claims out of a total of 530.6M total claims. So, over 5 years and with lots of effort, the number of mail claims has grown slower than the total claims growth. Some of this is due to client mix and plan design. Some of this is due to things like the $4 generic programs at Wal-Mart. But, how does this gel with the IMS data and the independent pharmacy complaints?
Or, is this due to the increased growth and focus on 90-day retail?
Sugar and Cholesterol
April 22, 2010 0 Comments
If you have high cholesterol, drink water NOT soda, juices, lemonade, sweetened teas, etc! That’s my quick summary of the article I read.
Of course we all know that sugar intake is linked to obesity which is linked with high blood pressure and heart disease. I think logically many of us would know that sugar is tied to cholesterol but generally the focus is on reducing fat intake. I simplistically think of it as the primary driver of my tricyceride levels.
Based on the study just published looking at over 6,100 adults:
- Participants consumed an average of 21.4 teaspoons of added sugars a day.
- 16% of participants total calorie intake was from added sugars (compared with 11% in 1977-78).
- People with higher levels of sugar intake were more likely to have low HDL and high triglycerides (blood fat).
The American Heart Association says that women should consume no more than 6.5 teaspoons of sugar a day and men no more than 9.5 teaspoons a day. [A Coke has 16.5 teaspoons in a 20 oz bottle or 10 teaspoons in a 12 oz can.]
HealthEngagement Barometer 2010
April 20, 2010 0 Comments
Edelman recently published the results of a survey of over 15,000 people across 11 countries.
The study is interesting in terms of people’s opinions. Here’s a few highlights.
- More than 50% of people believe businesses are doing a poor job of engaging in health.
- 73% say it’s as important to protect the public’s health as it is to protect the environment.
- 61% believe they need to do a better job of taking charge of their own and their family’s health.
- Only the UK reads and shares less information than the US. 41% of people read health information weekly and 33% share health information weekly.
So, what do people mean by how businesses should engage?
 One of the things that interested me was the slide about what motivates people to get active in their health.
One of the things that interested me was the slide about what motivates people to get active in their health.
 While 58% of people use some form of digital media to research health, the majority use Google or some search engine. 34% of them (globally) use health company websites. [If this were limited to health plan or PBM websites in the US, that would seem high.]
While 58% of people use some form of digital media to research health, the majority use Google or some search engine. 34% of them (globally) use health company websites. [If this were limited to health plan or PBM websites in the US, that would seem high.]
 I wasn’t surprised that fighting cancer was the most important issue, but I was surprised that privacy of information was the least important.
I wasn’t surprised that fighting cancer was the most important issue, but I was surprised that privacy of information was the least important.

Share This

My LinkedIn Profile

 WSJ Health Blog
WSJ Health Blog
- Is a Paleo Diet Healthier Than Standard Nutritional Guidelines?
- Small Business and the Affordable Care Act: How Has Your Business Been Affected?
- HealthCare.gov Explorer: Decode the Health Law’s Subsidies
- One Reporter, Four Families, Six Scientists and the Search to Cure a Rare Disease
- Your Responses: How Has the Health Law Affected You?
- What Does the Health Law Mean for You? Your Questions Answered
- How Has the Health Law Affected You?
- Rare Diseases and the Search for a Cure: A Reddit AMA
- Robots to Cure Rare Diseases: A Reddit Ask Me Anything (AMA)
- Six Tips For Better Napping
Drug Channels
- PBM Industry Update 2026: Trends, Challenges, and What’s Ahead (NEW Live Video Webinar)
- Time to Evolve: Hubs Flex to New Demands
- Preorder Now: DCI’s 2026 Economic Report on U.S. Pharmacies and Pharmacy Benefit Managers
- Beyond DTP 2.0: How Flexible Direct-to-Patient Programs Power Best-In-Class Patient Experiences
- Drug Channels News Roundup, February 2026: Mark Cuban on FTC-ESI, What Patients Really Want, QALYs vs. MFN, 340B’s Site of Care Shift, and New Faces at DCI
- The State of Patient Access: What Industry Leaders Reveal in a New Survey About Hub Models, Technology, and the Road Ahead
- Medicare Part D Pharmacy Networks in 2026: Supermarkets Dominate as Drugstores Stall and Independents Walk Away
- The Key to a Better Patient Experience: Improved GTN
- Copay Accumulators and Maximizers in 2025: Popular, Profitable, and Problematic
- In an Uncertain 340B Environment, Kalderos Offers a Clear Path Forward
KevinMD Blog
- An error has occurred; the feed is probably down. Try again later.
Health Populi
- Consumers Are Ahead of Consumer Health Innovation: Insights from IQVIA
- “Will Work For Health Care:” Americans Trading Off Wages For Healthcare (Again)
- Why Clorox Talks about Hygiene at Home: Health, Wellbeing, and the Home as Health Hub
- Dr. Wachter Bets on A Giant Leap for AI in Health Care
- Financial Stress and Trust in Health Care Takes Many Forms – Listening to Jarrard’s 2026 State of Play Survey
- Health Care Ads at the Big Game (Super Bowl LX) – Edgy, Entertaining, Educational
- When a Hotel Becomes Your Health Partner – Learning from Novotel and Accor
- The New (Old) Long-Term Care: Intergenerational, Together at Home
- The Healthcare Affordability Elections, 2026 and 2028 – Listening to the KFF Tracking Poll, January 2026
- Optimistic and Skeptical: How Older Americans Are Using and Seeing AI – the View from AARP
e-Patients
- Everylife Foundation Community Congress Annual Meeting Highlights
- Collaboration is the Best Medicine: Patient-Centered Collaboration Grounded in Caritas®
- Collaboration is the Best Medicine: It’s the Heart of Caregiving
- Collaboration is the Best Medicine: How to Partner with Your Doctor for Better Care
- Collaboration is the Best Medicine: Bridging the Gap in Patient Participation
- Dealing with Medical Uncertainty, Ambiguity, and Frustration
- Collaboration is the Best Medicine: The Time for Participatory Medicine is Now
- In Memory of Nancy Finn: e-Patient, Advocate, Author, SPM Supporter
- A cure for what killed Doc Tom! Can people afford it?
- Learning Health Systems Empower Every American to Actually Make America Healthy Again Together, Part 2

Enabling Healthy Decisions Blog by www.georgevanantwerp.com is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 United States License.

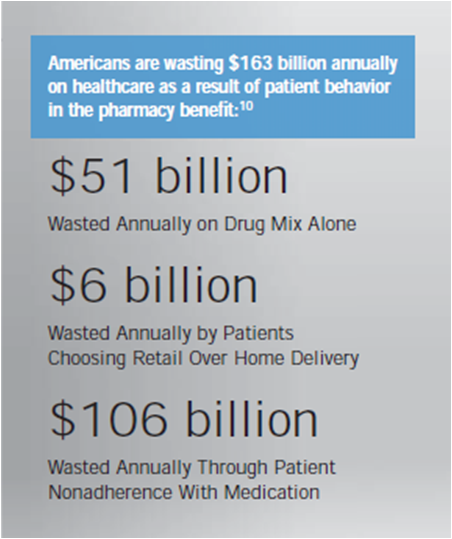{kind=link}
{kind=link}