
A new site I heard about is called VideoMD. Here’s one of the videos I found on it.
(But, I couldn’t use the embed code from their website so I used the embed code from YouTube.)
 November 22, 2010
November 22, 2010  0 Comments
0 Comments
A new site I heard about is called VideoMD. Here’s one of the videos I found on it.
(But, I couldn’t use the embed code from their website so I used the embed code from YouTube.)
November 21, 2010 0 Comments
Adam Fein was kind enough to send me an updated chart of the one I posted yesterday that comes from his new report “The 2010-11 Economic Report on Retail and Specialty Pharmacies” which will be available December 7th here – http://www.pembrokeconsulting.com/industry-reports.html.

One of the interesting things that isn’t clear in the industry is that while mail order made significant gains in the past decade, the IMS numbers show negative growth over the past few years. On the flipside, mail order numbers and new users are still a big focus across the PBMs. It begs the question of whether mail order growth without intervention programs is negative and only those with an effective retail-to-mail strategy can replace and potentially grow mail faster than people organically leave.
It also begs more discussion on the topic of retention which while a hot topic for a while hasn’t manifested itself in many rigorous programs as of yet (to my knowledge).
November 17, 2010 0 Comments
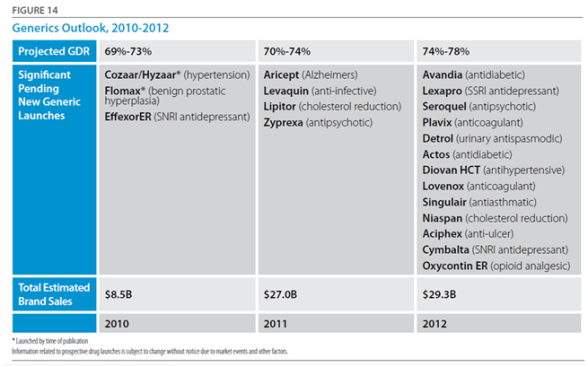
I’m catching up on a few things this week. One of those is sharing my notes from the CVS Caremark Insights 2010 publication (their drug trend report). While this year’s report outlines all of the traditional things you would expect – trend, spend by condition, market conditions, generic pipeline, I really thought the exciting information was at the end where they really begin to stitch together the retail / PBM model. I’ve talked about why I believe in this model so strongly in the past (you can also see some of their executive’s comments here). And, I think my perceptions about the future of pharmacists create lots of opportunity for a combined entity. I also think they hint at some of the insights they gained from research around non-adherence and around abandonment which is important and creates a foundation for them around predictive modeling and focused interventions.


“With overall goals of reducing health care cost and improving member outcomes, health plan respondents in our 2010 benefit planning survey placed high value on proactive member outreach (93 percent), multi-channel access for members (87 percent) and opportunities for face-to-face consultation (73 percent)—all factors that can help keep members on prescribed therapies and satisfied.” (page 14)

Member retention is critical and involves a balance of copay levels, premiums and drug coverage as well as less tangible factors. Member satisfaction plays a significant role in loyalty and re-enrollment. High-performing plans focus on effective member communication and outreach as well as added-value services such as the CVS ExtraCare Health card.

For a 1M member population, ~$12M is spent each year on 18 drugs that are administered to patients who do not respond and/or who are more likely to experience drug-induced medical complications.
“Diabetes is one of the most prevalent and expensive chronic diseases in the nation, costing the U.S. an estimated $174 billion a year,” said Troyen Brennan, MD, MPH, EVP and Chief Medical Officer of CVS Caremark. “The Pharmacy Advisor program improves clinical care because we are able to identify and address pharmacy-related care issues that if left unattended could result in disease progression and increased health care costs. We are also better able to engage the member in their care through multiple contact points, providing counsel that can improve adherence and help members optimize their pharmacy benefit and find the most cost effective options.” (quote from press release)

Overall, it was an easy read without a lot of fluff. It cuts to the chase and gives you a good perspective on how they think. You begin to get a feel for what they are doing differently, but I imagine that you’ll continue to see a lot more research and case studies come out in the next year about some of the work they are doing.
(Note: In the sense of disclosure, CVS Caremark is a stock that I own.)
November 12, 2010 1 Comment
I am way behind this year in getting thru the Drug Trend Reports and posting my comments. I think I still have to do both the CVS Caremark report and the Walgreens report…and if I can get it, the SXC report also. (You can see my thoughts from the Medco and Express Scripts Drug Trend Reports earlier.)
A few things I’ve found interesting this year were that Medco reached out via their PR group to engage me and several other bloggers in the space. And, Prime Therapeutics has always been very active in engaging me around my thoughts on their report (see comment from last year) and continued to be proactive in discussing it with me and sending me a hard copy to read on the plane.
Overall, I think their Drug Trend Report continues to improve year after year. It’s interesting in that this year I found the tone slightly more aggressive in talking about them versus their competition. Certainly, Prime is going thru some changes (if you haven’t noticed). They brought Eric Elliott on board who I think very highly of after hearing him speak and engaging him on a few topics. Eric has brought in a set of core people from Aetna, Cigna, Express Scripts, and other places to complement an existing management team that really understands the market and how to work with the Blues owners. [I personally think of them (and MedImpact or SXC) as a dark horse would could consider bidding on the Walgreen’s PBM lives while everyone is pretty focused on it being either Express Scripts or Medco.]


October 29, 2010 0 Comments
I was quoted in yesterday’s Drug Benefit News with one of my favorite people – Dr. Steve Miller from Express Scripts. This was a follow-up to talk about their predictive model for adherence. Steve confirmed what had previously been reported that it is 85% accurate in predicting the 10% of people least likely to be adherent. He says that the model takes into account past behavior, demographics, condition, and the drug. Those sound like a lot of the right variables.
The article teases us with information that CVS Caremark is planning to publish a study in the upcoming months on their model. Medco Health Solutions comes across as more of a skeptic in the article talking about efforts from 20 years ago that were difficult and expensive to execute.
My quotes were very consistent with what I’ve shared on the blog – fascinating, somewhat skeptical, more concerned about the group that is somewhat adherent than those that are the bottom 10%, implementation of behavior change is more important that the model.
“Everybody’s trying similar efforts in terms of how to predict adherence…but there hasn’t been a model that has proven itself as being a good predictor. Maybe Express Scripts has cracked the code…I would assume that if you can accurately predict who is going to be adherent that will be a good tool.”
However, attempting to change behavior in the top 10% of patients likely to be nonadherent will be tough, Van Antwerp contends. “The industry is still waiting for that proof,” he maintains. “If we can predict that patients are adherent but can’t change behavior, then the model doesn’t do us much good.”
October 21, 2010 0 Comments
I was fielding a few questions today about the predictive model from Express Scripts. The concept of predictive modeling is one that everyone is working on and holds great allure. BUT, it is only a piece of the puzzle. In the dialogue, I identified three key tenets for success.
And, then you need to study and refine these on an ongoing basis especially since topics like adherence may be affected by macro-economic trends (e.g., economy), patient beliefs (e.g., fatalism), and other attributes (e.g., plan design) on top of the attributes in your models.
I do believe we’re early in the days of modeling and that the access to data and greater availability of informatics resources will increase the development and focus on these models.
October 20, 2010 0 Comments
I liked the simplicity of the Walgreens’ ad that I saw this morning in a magazine (although I don’t like the tagline about “there’s a way to stay well” since there is a healthcare company named StayWell).
It provides this series of data points:
70,000 healthcare professionals
25,000 certified immunizing pharmacists
7,560 community pharmacies
1,670 physicians, nurse practitioners, and physician assistants
900 infusion nurses
700 worksite health centers and convenient care clinics
125 medical facility and specialty pharmacies
100 infusion and respiratory centers
1 Walgreens
October 20, 2010 1 Comment
I always get pulled into the discussions about what PBMs are doing, should be doing, or could be doing in social media. For now, let’s just look at the current state – i.e., who is doing what.
I’m going to focus on the big channels – Twitter, Facebook, YouTube, and blogging.
To make it easy, I created a Twitter list on my profile of the PBMs, pharmacies, and several other key resources in this area – http://twitter.com/#!/gvanantwerp/pharmacy-pbm.
I welcome your links to other PBM or pharmacy social media assets. I looked under CatalystRx, Prime Therapeutics, and SXC also. I also checked Cigna Pharmacy, Humana Pharmacy, Prescription Solutions, and Kaiser Pharmacy. I couldn’t find more, but I’m sure there’s a few I missed.
The question of course is how to judge if these are successful. Is it the number of followers or fans? I would argue no. The goal of social media is to create a dialogue and engage the patients or consumers. Given the traditional focus on the PBM on the business-to-business relationship and the pharmacy on the business-to-consumer relationship, there is an interesting question of how the mail order pharmacies (owned by the PBMs) make that leap. Can social media create a forum for discussion about plan design, drug trends, and other things in straightforward language that engages consumers? Will consumers be willing to use these channels to interact with the PBMs or only with their pharmacist? This could be an area where companies like Walgreens or CVS Caremark who have a large physical footprint can leverage a real-world connection with consumers to a virtual one easier than others.
As you can see, there are not a lot of people doing a lot yet. This area will change a lot in the next 5 years.
October 18, 2010 0 Comments
I came across this framework that I like. It seems to take into account the health literacy and emotional challenges of a patient when receiving and assimilating bad news.
COMFORT stands for:
Communications – use clear and familiar language.
Orientation – set reasonable expectations.
Mindfulness – focus on the patient without being distracted.
Family – include the family in the information and the ongoing support.
Ongoing – stress the ongoing activities so there is no sense of abandonment.
Reiterative – continue to reinforce the message to help them come to terms.
Team – coordinate care so that there is not conflicting or confusing information.
October 15, 2010 0 Comments
Communications continue to evolve. Mobile health in the form of applications has either crossed the chasm or is crossing the chasm. I expect in 5 years that most communications in healthcare for people under 45 will start with a mobile application. It may “escalate” to other modes, but using a secure application on the ubiquitous mobile phone will be a primary starting point to engage them.
Caremark rolled out their mobile application earlier this year. Now CVS has rolled out there application. Several other companies have rolled out their applications also. Humana’s application is out (mobile site). Another big PBM is piloting their mobile application with one employer right now.
So, what does the CVS mobile application do:


October 15, 2010 0 Comments
I can’t believe I missed this one earlier this year especially since a friend of mine is one of the authors…BUT this is an important one for the industry showing that not only did adherence improve moving from retail to mail order pharmacy but as pharmacy costs when up the corresponding medical costs went down MORE!
I’m just going to paste the abstract from the Journal of Medical Economics below:
Objective: To compare long-term diabetes medication adherence and healthcare costs in patients using mail order pharmacy versus retail pharmacy.
Methods: The MarketScan database was used to identify patients who filled prescriptions for oral anti-diabetes medications in a retail pharmacy for at least 6 months before switching to mail order pharmacy for at least 12 months. These patients were matched to others who used retail pharmacy continuously for at least 18 months. A propensity score was used to create matched groups of patients comparable on probability of switching to mail order, weighted Poisson regression was used to analyze differences in medication adherence, and Tobit regression was used to compare costs.
Results: A total of 14,600 patients who switched to mail order were matched to 43,800 patients who used retail pharmacy continuously. The average adjusted adherence in retail pharmacy was 63.4% compared to 84.8% after switching to mail order. Per-member-per-month total healthcare and total medical costs were on average $34.32 and $37.54 lower in the mail order group, respectively. Diabetes-related medical costs were on average $19.14 lower in the mail order group, while pharmacy costs were $14.13 higher.
Limitations: Limitations include a patient population under the age of 65, no information on pharmacy benefit design, and limited follow-up time relative to that necessary to identify long-term diabetes complications.
Conclusions: After adjusting for measured confounders of medication adherence and disease severity, individuals who switched to mail order pharmacy had higher medication possession ratios and trended toward lower total and diabetes-related medical costs over time.
Press release about it here.
Here’s a slide showing the values:

October 15, 2010 0 Comments
I was looking at the latest investor decks from Express Scripts on their site and found this slide in the presentation from the William Blair Growth Stock Conference. It does a nice job of comparing the two channels although I’m sure that my retail friends would hotly debate this topic.

October 14, 2010 0 Comments
I’ve talked about this with many clients. Since physicians don’t always engage patients in the basic dialogue around adherence, how can they decide to increase doses or change prescriptions simply if the patient’s condition isn’t becoming better? This has to drive waste in the system.
The reality is that a physician may get a lab value that shows that their patient’s cholesterol (or A1c or…) is higher than it was last time. They know the patient is on a certain dose of the medication. They instinctively think to increase the dose or change the medication. BUT…they don’t always ask the patient about their adherence to the medication. This is attributed to multiple reasons:
I’d heard about a study done about a decade ago that had looked at this, but it had never been published. I was excited to see that Medco had published some research on this topic today.
There were some interesting things in the research also. It was another validation on the fact that men are more adherent than women. And, it showed that people with multiple conditions were more adherent. I would expect that there is a curve around this that people with a few medications and those with lots of medications are least likely to be adherent, and those somewhere in the middle are most adherent. (But, I’ve never looked at the data with this question in mind.)
October 13, 2010 1 Comment
The Medicare Part D prescription drug coverage has been a great validation for the PBM industry. It has shown the ability of the traditional tools to manage spend and provide an affordable benefit.
With that said, a new survey conducted on behalf of the Medicare Today coalition shows more reinforcing data:
“The Medicare Part D program continues to defy its doubters,” said Mary R. Grealy, president of the Healthcare Leadership Council and co-chair of Medicare Today. “At its outset, critics said health plans wouldn’t participate in Part D, but today seniors have ample choices of affordable plans. They said the program would cost too much, but the last Medicare trustees report reported costs are 41 percent below initial expectations. And they said seniors would find the program too confusing, but it remains enormously popular.”
October 12, 2010 0 Comments
One of the things all of us do is present. Steve is a genius at this. If you haven’t looked Presentation Zen and seen Jobs present, here’s a few points from a deck I found…
October 12, 2010 1 Comment
More and more, I am getting in conversations with clients about emerging media and how that plays into their healthcare communications strategy. Whether that is simpler things like PURLs, SMS, and mobile applications or more complex decisions around Twitter, Facebook, YouTube, blogging, and social media.
Here are a few things from YouTube that I thought were good on the general market.
October 12, 2010 0 Comments
There is lots of buzz over yesterday’s article in the WSJ about Express Scripts being able to predict who will be adherent. Today’s blog post on the Corporate Research Blog added some details (or further confused me). It says that the model is 80% accurate in predicting the 10% of people who are least likely to be adherent.
Is that all it does? For sake of this post, let’s assume it does. That seems much less interesting and much easier to do. In talking with a leading researcher in this area that has looked at the correlation of 9,000 variables to adherence, he told me that nothing was highly correlated, but the most correlated metric was past behavior. Where they adherent in the past on other medications? Did they take preventative action (e.g., get flu shots, mammograms)?
Several people have been looking at how credit scores can be used to predict adherence. Given errors in credit scores, this may be deceptive even if it works.
But, back to the issue. If you know who’s least likely to be adherent, so what? Do you give up on these people? They aren’t likely to chance behavior. Do you try harder or have a different strategy with these people? If you succeed and move them to taking their medications 40% of the time (using a proxy like a 40% medication possession ratio), does it make a difference?
I would think it’s better to focus on the people who are likely to be adherent and how to enable them to move from 40-70% MPR to >80% MPR. We often work with clients to stratify their population and have different intervention strategies (channel, messaging, level of effort, etc.) across where they fit in the model (value, likelihood to engage, likelihood to change).
October 7, 2010 0 Comments
Next week in DC is The Forum 2010 which is the annual event for The Care Continuum Alliance (formerly known as The Disease Management Association of America). If you’re there, you should stop by the Silverlink booth and attend the presentations that we’re giving with some of our clients and other industry leaders.

| Aligning Employee, Employer & Provider Research to Maximize Value-Based Benefits October 13, 1:00 – 2:00 p.m. Jan Berger, MD, MJ, Chief Medical Officer, Silverlink Communications Cheryl Larson, Vice President, Midwest Business Group on Health (MGBH) |
|
| Improving Statin Adherence through Interactive Voice Technology & Barrier-Breaking Communications October 13, 2:15 – 3:15 p.m. Ananda Nimalasuriya, MD, Chief of Endocrinology & Complete Care, Kaiser Riverside George Van Antwerp, MBA, General Manager, Pharmacy Solutions, Silverlink Communications |
|
| Addressing Colorectal Screening Disparities in Ethnic Populations October 14, 12:30 – 1:30 p.m. R. Reid Kiser, MS, National Director, Clinical Excellence Special Projects and Reporting, UnitedHealthcare Jack Newsom, MBA, MS, ScD, Vice President, Analytics, Silverlink Communications |
|
| Addressing an Epidemic – Improving Diabetes Care with Personalized Communications October 14, 3:00 – 4:00 p.m. Jan Berger, MD, MJ, Chief Medical Officer, Silverlink Communications William Shrank, MD, MSHS, Instructor, Harvard Medical School and Associate Physician, Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital |
October 5, 2010 0 Comments
Years ago when I was at Ernst & Young as a consultant, several of the partners wrote a book called BLUR. The concept (that I took away) was that products and services were being combined into offerings. That one could not stand without the other. A quick example for me is General Motors with OnStar, but there are numerous examples out there.
In pharmacy, I think this has been the standard around specialty drugs for years. Manufacturers produce the drugs and sell them to a pharmacy for distribution. With that, they provide educational materials, adherence programs, or other “services”.
I think going forward that there is going to be increasing need to differentiate even oral solids (traditional small molecule products) that are less expensive and focus on chronic conditions. Formularies are only going to get more narrow. Comparative effectiveness is going to push companies to compare overall outcomes of products. Why not find a way to wrap a similar service strategy around these medications in a more technology driven, scalable manner?
It seems like a great way to show that not only is your product effective when taken, but that patients on your product are more engaged with their condition and more likely to stay adherent.
October 5, 2010 0 Comments
Metabolic Syndrome…does that mean anything to you? I doubt it.
Here’s the official definition (and a good summary here), but in layman’s terms, it means you’re obese and at risk for many different health conditions.

Metabolic syndrome is a combination of medical disorders that increase the risk of developing cardiovascular disease and diabetes. (definition and picture from Wikipedia)
I just find this a classic example of us (healthcare people) creating and then using a medical term to describe something that simply obfuscates the problem that someone is overweight.
September 30, 2010 0 Comments
This one intrigues me. We know that it’s much easier to convey emotions face-to-face…BUT we continue to evolve to more electronic communications and less face-to-face interactions. So, does that lead to more mis-understandings. I’m sure it does. One study says e-mails are mis-understood 50% of the time.
Haven’t you ever read an e-mail several times trying to figure out what the writer was trying to say and making certain assumptions. We all read into messages.
The application is ToneCheck which integrates right into Outlook. I haven’t tried it yet, but I’m intrigued by the demo.
September 30, 2010 0 Comments
This new study says that just holding an alcoholic beverage makes you seems stupid. While I would agree that if your Facebook picture or blog picture was you with an alcholic beverage, I might think twice, but I’m not sure I would have the same impression of a person at a reception with a glass of wine.
But, it made me think about how important it is to think about images as aligning with messaging and branding. This is important in direct mail and e-mail and on the Internet. Being in the communication business, we often bring in mis-aligned marketing pieces to share with each other. (Maybe there needs to be a bad marketing blog like the bad pitch blog.) I remember one from a few months ago which was a happy birthday postcard to someone on turning 40 and encouraging them to take some action. The image on the postcard was of a 70+ year old woman. It really made the woman turning 40 feel like it was older than it is.
In another case, I think about when I was an architect. We were designing a boardroom for a big Fortune 100 company. When we were creating a rendering for presentation, I was told that the CEO didn’t like to see women in the pictures (probably wouldn’t happen these days) so we could only add images of men in business suits to the pictures.
September 27, 2010 0 Comments

Do you brush your teeth more before you go to the dentist?
Are you more likely to take your medications the week before you go back for your physician visit?
YES!
But, do we make that clear to the physician? No. When the physician asks if you’re taking your medications, the answer is yes. That’s not a lie. What they need to know is how many pills are left since you last filled your medication? How many pills did you start with? How many did you lose?…
You get the picture. I like the term here that our Chief Medical Officer used – “white coat adherence”.
Now, let’s imagine that the physician orders a blood test for your cholesterol and your LDL hasn’t dropped, there are three scenarios:
1. They go back and really push you on your adherence (or diet and exercise);
2. They believe you but they assume the medication dose isn’t strong enough and increase your dose; or
3. They believe you but they assume the medication isn’t working and change your medication.
These are minimally issues for the healthcare system – wasted costs – but there is also the potential for giving you an unnecessarily high dose or changing you to a riskier medication since the default one didn’t work.
How do we address this? It’s not easy. This involves a few things:
1. Improving physician access to data (i.e., adherence data);
2. Improving physician – patient communications; and
3. Helping patients stay adherent and understand the impact of their medication (and lifestyle decisions) on their health.
I continue to see more and more data on the physician patient gap in communications. This is from a few years ago, but a study showed that 40 to 60% of patients could not correctly report medication expectations 10 to 80 minutes after physicians provided information, AND more than 60% of patients misunderstood prescription directions immediately after doctor visits. (source)
Pretty scary!
September 23, 2010 1 Comment
Per my prior two posts on this, Drug Benefit News (DBN) published an article today on this topic. Renee talked with me along with several other people to get a perspective on the topic.
Here are a few quotes from the article:
“Auto-refill for prescriptions is all the focus lately,” says George Van Antwerp, General Manager of Pharmacy at Silverlink Communications. “Everyone from the big PBMs to the local pharmacies are encouraging this.” This is because auto-refill programs address one of the common patient-reported issues with adherence — forgetfulness — allowing insurers to “minimize gaps in care.” Auto-renewals, on the other hand, are not considered common practice and many payers are hesitant to implement the service.
Express Scripts, Inc. is one of the few PBMs developing an auto-renewal program, which it will offer through home delivery. “Renewals are much more problematic than refills for patients when procrastination occurs,” Bob Nease, Ph.D., chief scientist at Express Scripts, tells DBN. “If you procrastinate on getting a renewal, it’s not just a matter of calling the pharmacy. You have to get a new prescription with a physician. And if you talk to physicians, they pull their hair out over this issue.”
Others contend that auto-refill and renewal programs may up plan costs by increasing medication waste. The concern is that auto-renewals may result in “provisions of medications that may not be a current active medication therapy or where the patient may have experienced an adverse effect and their drug therapy may have been modified by their physician,” contends Andy Szczotka, senior vice president of corporate clinical services at HealthTrans. “This may lead to potential medication waste and increased member and plan sponsor costs.”
“This is all done under the assumption that you’re improving adherence,” [Jerry] Shipkin [from SXC] says. “But I have not seen solid evidence that this improves adherence.”As an alternative, SXC sends its members auto-reminders with phone calls or e-mails to inform patients about their upcoming refill. “This is a more patient-friendly program,” Shipkin argues. “When you measure patient adherence on this program, it’s just not significantly lower than what you might get on an auto-refill program when you calculate the reversal.”
Van Antwerp contends that auto-reminders aren’t enough. “Everyone does auto-reminder programs,” he says. “In my mind, that’s the minimum that a pharmacy or PBM should do.”In addition, he argues, “anything can lead to accumulation if the patient is not using their medication and refilling their drug on a regular basis.” However, “how many patients do that?” he asks. “Drugs cost money.” While it could drive up more prescriptions, “no one’s going to pay for — and/or pick up — scripts they don’t need,” he maintains.
CVS Caremark Corp. claims its “Ready-Fill” program is “a convenience our members love,” according to Bari Harlam, the PBM’s senior vice president of marketing. The program includes auto-refills and auto-renewals. “There are a lot of people that have trouble being adherent, and this is a service that we offer to our consumers that helps do the work for them,” she tells DBN.
CVS Caremark members enrolled in the program receive notifications about their refill a few days before it’s shipped, and have the option of cancelling the refill. The PBM also calls its members’ physicians to request additional refills. “The physicians’ offices view this as part of the normal workflow, and retail and mail pharmacies are always reaching out to them for particular medications,” Harlam says.
September 23, 2010 3 Comments
The study came out yesterday. I pulled the data from the executive summary into a powerpoint for all you visual people like me. Some interesting statistics on the value of pharmacy satisfaction and retention. Maybe this will create the business case for more tracking and focus on impacting satisfaction in pharmacy. I think we’ve seen that over the past few years for managed care with individual insurance.
Before you peek, who (pharmacy type) do you think gets the highest average ranking in satisfaction?
September 21, 2010 0 Comments
I can’t seem to find a lot of infographics on pharmacy (which is surprising to me since I find the space so fascinating). Here’s one I found in a Fast Company article.

September 16, 2010 3 Comments
A few weeks ago, I posted my thoughts on the auto-refill solution that various pharmacies are implementing. After talking with a reporter about the topic, I posted it in a discussion group to get some additional thoughts. As a proponent of the solution, I was surprised by a few of the comments and questions which were more skeptical.
With that in mind, I thought I would post some clarifications to the issues raised in the discussion group.
You can see more dialog on this at The Pharmacy Chick blog or in this article from last year.
“Steven Friedman, VP of pharma services at PDX-Rx, notes that the company’s dispensing and adjudication software, when engaged for auto-refill, has been shown to add as much as two additional months on therapy (i.e., two more months of adherence) in a six-month period—a substantial improvement both in adherence and in pharmaceutical sales.”
What’s the net of all this (IMHO)…
September 11, 2010 0 Comments
Medication and health management strategies are integral parts of patient care, but if those who need medical help can’t understand their instructions perfectly, the right procedures are lost on them. Health literacy is a growing concern, and it refers to one’s ability to read, process, and implement directions related to personal health care. Both the context of health-related communication and the skill level of health care providers are strong factors in health literacy, but it ultimately describes the comprehension abilities of someone on the receiving end of health care. In a study conducted by Dr. David Baker, MPH, and a team of researchers, it was found that inadequate health literacy contributes significantly to mortality rates among the elderly.
Health Literacy and Mortality Findings
Baker and his team administered a shortened version of the Test of Functional Health Literacy in Adults to a pre-screened cohort of 3,260 Medicare managed-care enrollees. They then collected their data and categorized it into three sections: adequate, marginal, and inadequate health literacy. These results were then compared to all-cause and cause-specific mortality data from the National Death Index, 1997-2003. Although the category of elderly patients with adequate health literacy accounted for the majority of the cohort at 2,094 individuals, their mortality rate averaged only 18.9%. The group with marginal health literacy, which included 366 individuals, averaged a mortality rate of 28.7%, and the group with inadequate health literacy at 800 had a 39.4% mortality rate. Baker and his team found that the number of years of school completed by the subjects was barely associated with mortality, leaving reading and comprehension abilities as the main indicators in determining health literacy. A general lack of health-related knowledge, the ability to apply it, and wide variety of other “pathways” characterized those individuals with inadequate health literacy.
Ways to Address and Manage Health Literacy
According to health.gov, a page dedicated to the activities of the U.S. Department of Health and Human Services and other Federal departments and agencies, there are many ways to develop and deliver health information while maintaining awareness of health literacy. For example, information should be appropriate for the user audience and easy to use. It’s also important to speak clearly and listen carefully when communicating health-related information. The following are some strategies that may help pharmacists, doctors, and other health care professionals communicate information clearly to non-professionals and patients.
Guest Blogger: Alexis Bonari is a freelance writer and blog junkie. She is currently a resident blogger at First in Education, researching online college degrees. In her spare time, she enjoys square-foot gardening, swimming, and avoiding her laptop.
September 10, 2010 0 Comments
Let’s start with a few facts:
Retailers (and likely others) are trying different things to drive flu shot volume:
This year, the competition for administering flu shots will be aggressive among retailers:
Walgreen says it administered 7.5 million H1N1 and seasonal flu shots last season, up from 1.2 million the year before. Walgreen’s figures represent about half of all the retailer-administered flu shots, says Mr. Miller, the analyst. He estimates retail pharmacies could administer 20 million to 30 million flu shots this season. Rite Aid, which doled out 250,000 shots last year, said it has ordered a million doses for this year.
Grocery chains with pharmacies also are pushing flu shots harder. Supervalu Inc., operator of the Jewel, Shaw’s and Albertson’s, says it expects to deliver 50% more flu shots this year in its 800 pharmacies. Kroger Co., the second largest food retailer by sales, says it will have flu vaccines available in all of its 1,900 pharmacies. (From WSJ)
The logical question would be why would the pharmacies care. Money. Flu shots are a profitable business and as long as you can administer them without disruption to your workforce…then your variable costs are limited. But, that also makes me wonder why everyone is taking a general marketing approach. There is lots of marketing, but very little targeted marketing that I’ve seen around flu shots (from the retail community).
On the flipside, managed care companies have a totally different reason to drive flu shots – it’s a HEDIS measure. [And, BTW…HEDIS is a big part of the STAR Ratings that CMS is using to pay incentives to Medicare plans.] They want to limit sickness, hospitalizations, and other medical costs.
This is one where everyone is aligned so that employers also want to drive flu shots to avoid absenteeism from sick employees. This article puts the value of a flu shot to the employer at $46.50. Since flu shots cost less than $30, why wouldn’t employers just give everyone a free flu shot. They’re getting a 50% return on their investment.
A more interesting debate is whether to mandate flu shots in certain cases. The biggest one which is debated is healthcare workers (although I would also lump in teachers and day care staff). The last thing you want is someone who is already at risk and sick to be exposed to the flu when they go to receive care.
Last January, a CDC survey found that just 37% of health care workers received swine flu vaccine and 35% received both seasonal and swine flu shots. On average, flu vaccination rates hover under 50%. (USA Today article)
So, I guess my net-net here is that flu shots are going to be pushed this year. I would think pharmacies and employers and pharmacies and MCOs would pair up to drive shots to specific locations. I think the general marketing and news will increase awareness, but the question is how to you reach the at risk population and drive them to your location and get them to get the shot early before they get exposed. I don’t think a build it and they will come strategy will “win” here.
[BTW – Every Google search I did around flu shots, brought back a Walgreens link at the top of the page.]
And, if you’re interested in what we’re doing or could do around flu shots at Silverlink Communications, let me know. (Here’s an old article on results.)
September 9, 2010 0 Comments
I remember a few years ago when I got my first text. It was from the CTO at Accenture, and I had a phone that didn’t have SMS. I had to click thru a link to a website to see the text. I was totally flustered. How was I supposed to respond?
Well…I’m past that now. My brother and I send happy birthday via text. I find it easier to send a quick text when in a loud spot like the airport than to try and call. I’m sure my volume is still low. My friend said their kid did 15,000 in one month (which seems impossible). Another friend told me that their kids can text without looking. They sneak a quick peak and then respond without even pulling it out of their pocket (when their supposed to be off the phone).
We all know this is an emerging communication channel that will continue to evolve. And, smart phone use and adoption is expanding rapidly. So, here’s the infographic.




