In today’s economy, the last thing we want to do is scale up a company by simply adding people. Technology has to play a central role in allowing you to grow your company more efficiently.
At the same time, you want to grow without dropping your level of service. You want to improve the consumer experience.
And, to further complicate matters, you have to manage quality both to make sure that you comply with regulatory oversight and achieve goals around first call resolution. With our rapidly changing healthcare environment and legacy systems in many places, finding, training, and retaining good staff that can continue to keep up with the changes and understand the semantics between plan designs isn’t easy.
So, how do you do that? You’re in a balancing act between cost, quality, and experience.
This is one of the big areas where I’ve seen Silverlink Communications play a role. (Note: There are certainly other efforts which you can undertake in terms of single desktop and process reengineering, but I usually refer in some people I trust for those projects.)
Some people call our technology a “smart dialer”, but there is a difference. If you ever get a call at home from a call center using a dialer, you hear that silence after you say “hello”. The technology is looking for an agent to connect you with. On the flipside, if you’re an agent, you’re being connected with someone or even an answering machine that might not be the right person. That’s what a dialer does.
In our case, Silverlink is using mass personalization, voice detection technology, and speech recognition technology to screen the recipient for the call center. You hear the message right after you pick up the phone. It’s a message that has been carefully crafted using behavioral sciences and health literacy. It asks for you by name and identifies who’s calling for you. It then confirms your identity, and depending on what information is being used in the call, it may have to use multiple forms of authentication to verify who you are. Once we’ve assessed who you are (based on your responses), we’re able to deliver a personalized message to you about your healthcare. That personalized message is scripted in such a way to engage you in a conversation. During that conversation, we can then determine:
- Are you interested in learning more?
- Is this a good time for you to talk?
- Would you like to talk to an agent or hear more now?
- Would you like us to send you information in an e-mail, SMS, or snail mail?
- Would you like a URL to go to for more information?
Occasionally, people ask about authentication. When you send a piece of direct mail, it’s a federal offense to open it if you’re not the intended recipient, but you have no proof that they did that unless your “nanny cam” picks it up. When you call someone, you have a record of when the call was made and what they person who picked up the phone said to authenticate themselves. This certainly seems better to me than any other channel.
Of course, this begs the question of recording all the calls. I’ve heard a few people tell me that they do this with other companies. I find that hard to believe since 12 states have consent laws which would require people to consent to being recorded when they were called. That would limit the effectiveness of the program, or if you didn’t do it, it would open you up to a big lawsuit.
So, how does Silverlink add value to a call center:
- Improving agent productivity. Automating standard questions. Connecting with the right person at the right time.
- Improving consumer engagement. Using behavioral sciences and health literacy to engage people and route them to the right agent based on skill set.
- Improving quality and consistency of experience. Personalizing the experience to engage the consumer but doing it in a way that addresses the clinical guidelines, regulatory requirements, and custom client requests in a consistent manner.
- Improving agent satisfaction. Your agents would rather talk to pre-qualified people or people who have an issue.
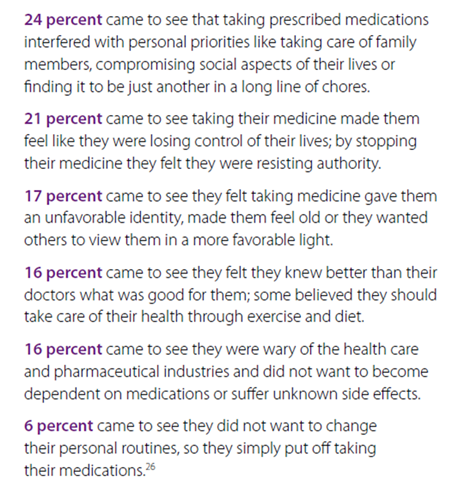
- Learning new information. In some cases, patients feel judged when people ask them questions (why aren’t you taking your medications). They may reveal more or other information in an automated environment.
Of course, automated calls aren’t the answer for everyone (although they work better than any other mode other than people…and sometimes beat them also). But, multi-channel coordination is a post for another day.

 April 13, 2011
April 13, 2011 



 Last week, I got to see one of the more interesting presentations I’ve seen in a while.
Last week, I got to see one of the more interesting presentations I’ve seen in a while.